


“The good physician treats the disease; the great physician treats the patient who has the disease.” Sir William Osler
“Listen to your patient, he is telling you the diagnosis.” Sir William Osler
Précis: The medical term used for excessive drooling is sialorrhea [si·al·or·rhe·a (sī-ăl′ə-rē′ə)]. Hockstein et al. said, “Sialorrhea (drooling or excessive salivation) is a common problem in neurologically impaired children (i.e., those with mental retardation or cerebral palsy) and in adults who have Parkinson’s disease or have had a stroke” [Hockstein NG, Samadi DS, Gendron K, Handler SD. Sialorrhea: a management challenge. American family physician. 2004;69(11).]. Drooling is a common symptom of Parkinson’s, which you can imagine would be a very awkward scenario in social settings. This blog post is to introduce the topic of how we produce saliva, why people-with-Parkinson’s may develop problems with drooling, and some strategies/treatment options to reduce it.
“Medicine is a science of uncertainty and an art of probability.” Sir William Osler
Start to the story: Several years ago I was sitting in IP3’s, the iconic pizza restaurant in downtown Chapel Hill on Franklin Street. IP3 is short for Italian Pizzeria III, which is a Family-owned restaurant where everyone is in the kitchen cooking together, speaking Italian with raised voices. However, as you enter the restaurant, they all turn and uniformly shout-out a sincere welcome. Upon serving pizza at our table, someone laughingly asked me “Frank! Did you just drool on the pizza?” And I said “No way! I drooled on the pizza? But if I did, I’m really sorry. I guess that will be my first slice.” Of course, now I’m thinking to myself, ‘geez Frank, you just drooled all over the pizza, what is going on?’ This began one of the first symptoms of my Parkinson’s long before it was ever diagnosed.
“The practice of medicine is an art, not a trade; a calling, not a business; a calling in which your heart will be exercised equally with your head.” Sir William Osler
Please Don’t Spit on the Floor: According to BBC’s Science Focus, swallowing is something that we do every day; and we do it mostly without even consciously thinking about swallowing. Actually, we swallow ~1000 times per day. Most of the time we’re swallowing saliva. We swallow ~30 milliliters of saliva per hour, which translates to filling up an empty bottle of wine every day.
Saliva is a hypotonic solution (this means it’s mostly water, not a lot of other stuff). Saliva is really here to help out the digestive, and immune systems do their jobs better. Really? Yes!
•It lubricates and cleanses the oral cavity using its water and glycoprotein content;
•It also controls bacterial flora by the action of lysozyme (it chews up bacterial cell walls), lactoferrin (it binds iron that bacteria want to use for energy), and immunoglobulin A (a type of antibody, which is part of your immune system);
•It initiates digestion of carbohydrates by the action of salivary amylase;
•It acts as a solvent for substances that stimulate the taste buds;
•And, it assists in the process of deglutition (swallowing).
“We are here to add what we can to life, not to get what we can from life.” Sir William Osler
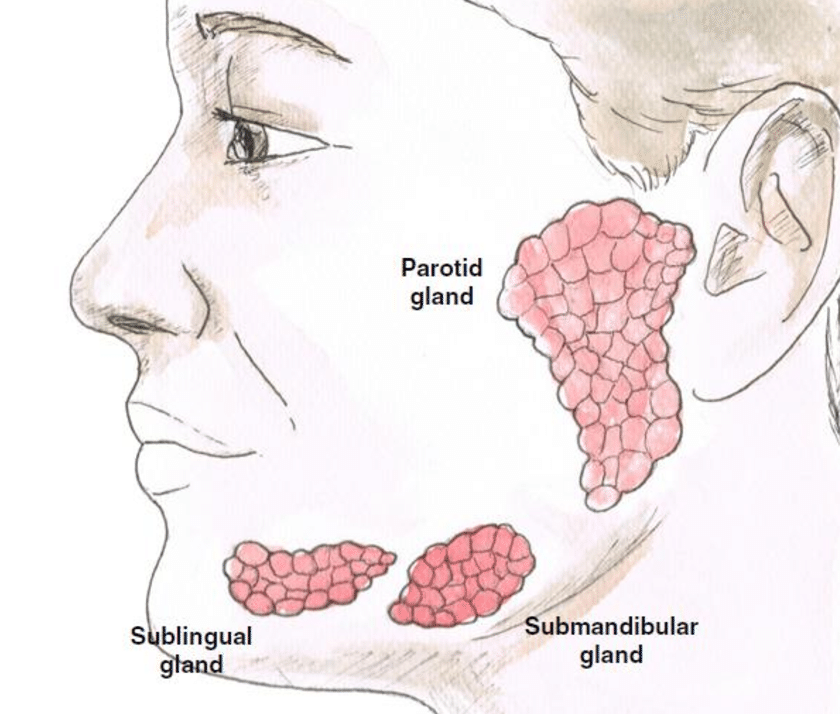
Salivary Glands and Swallowing: The picture below highlights the digestive system, and outlined in the red box is the region that begins digestion. The major salivary glands consist of three paired exocrine glands (exocrine glands are glands that produce and secrete substances using a duct), the parotid, submandibular, and sublingual (see 2nd figure below).
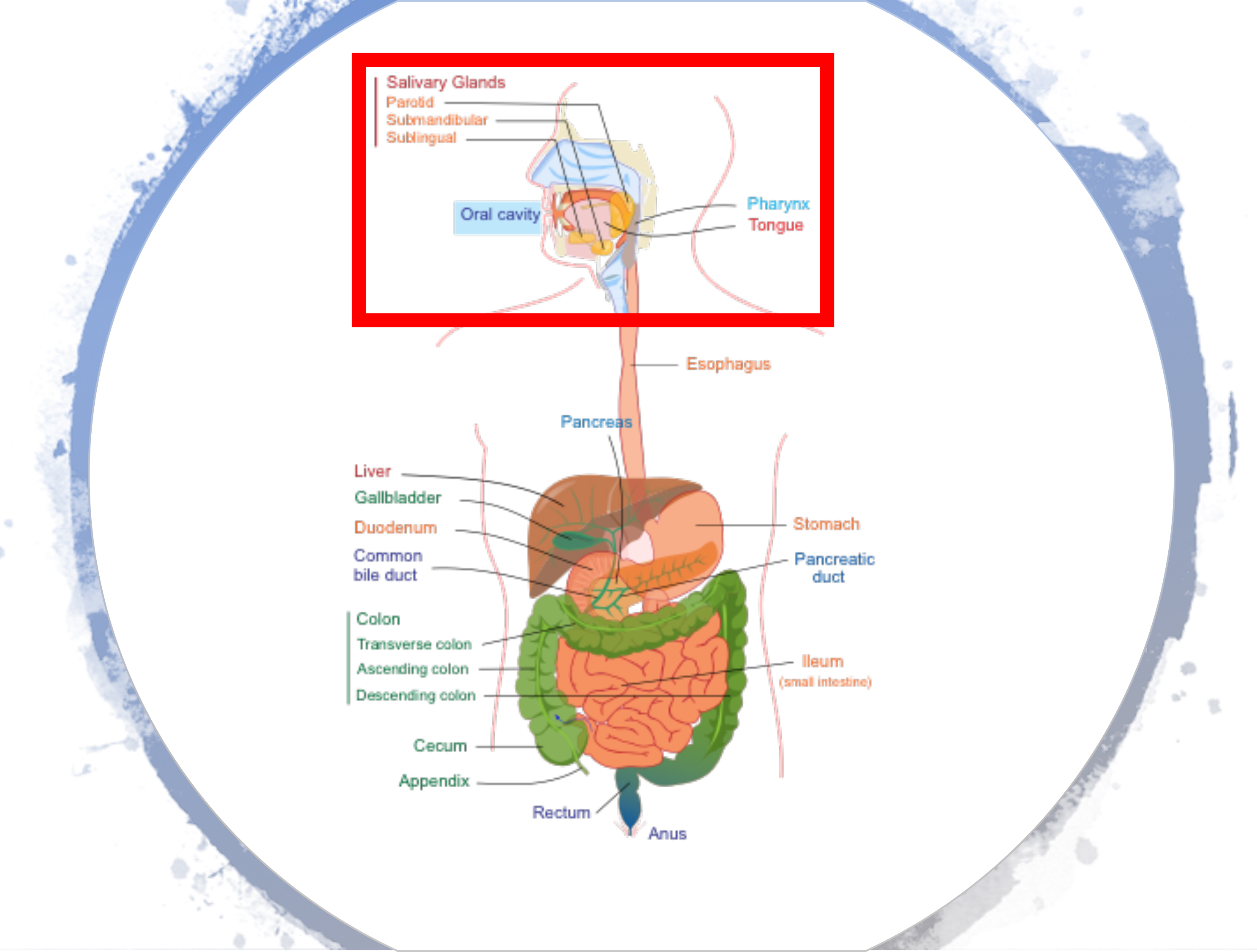
The submandibular glands are found located beneath the lower jaw. Approximately 65-70% of saliva in the oral cavity is produced by the submandibular glands. The saliva they provide is a mixture of both serous fluid and mucus. The parotid glands are the largest of the salivary glands. The saliva they secrete facilitates chewing and swallowing; it also contains an enzyme named amylase that begins the breakdown of starch in the food. They produce ~20% of the total salivary content in the oral cavity. The sublingual glands are a pair of major salivary glands located under the tongue, near the submandibular glands. The saliva produced is mainly mucus; ~5% of saliva entering the oral cavity comes from these glands. [Click here for more information.]
Active swallowing is dependent upon the precise timing of three primary phases; coordinated by the effective performance of many nerves and muscles:
•Oral Phase. Food is chewed and mixed with saliva to form a soft consistency called a bolus. The tongue then moves the bolus toward the back of the mouth.
•Pharyngeal Phase. The vocal cords close to keep food and liquids from entering the airway. The larynx rises inside the neck and the epiglottis moves to cover it, providing even more airway protection.
•Esophageal Stage. During the final stage, the bolus moves into the esophagus, the muscular tube that contracts to push the bolus into the stomach.
It is beyond the scope of the current post, but controlling the swallowing process is the autonomic nervous system (ANS). The ANS is a control system that acts mostly unconsciously and regulates bodily functions such as heart rate, digestion, breathing, pupillary response, urination, and sexual arousal. The image below demonstrates the complexity of the simple act of swallowing.

“Variability is the law of life, and as no two faces are the same, so no two bodies are alike, and no two individuals react alike and behave alike under the abnormal conditions which we know as disease.” Sir William Osler
Parkinson’s and Drooling: It has been estimated that ~50% of people-with-Parkinson’s have sialorrhea (excessive drooling). It has varying degrees that range from mild dripping on your pillow during sleeping to an outpouring of saliva while speaking. It frequently happens when you are doing something that requires concentration, and you are distracted from the function of swallowing. What? Why? Parkinson’s affects the ANS nervous system as mentioned above; the automatic part of our nervous system we don’t think about doing these bodily functions. It is believed that we produce an average amount of saliva, but we just do not swallow enough to clear it out. Thus, the loss of dopamine leads to the slowness of these muscles working to swallow and their increased rigidity; combined with the loss of coordination yields pools of saliva not being routinely cleared.
“The person who takes medicine must recover twice, once from the disease and once from the medicine.” Sir William Osler
Treating and Managing Drooling with Parkinson’s: If you are dealing with drooling, and yes, besides being a nuisance, it could mean complications of your Parkinson’s due to swallowing. Definitely, consult with your Neurologist or Family Practice Physician, and get referred to a Speech-Language Pathologist. You have several options, see what works for you, OK? Here are a few things to consider as noted by the experts (see the cited papers below):
•Chew gum or suck on hard candy because they can activate your jaw muscles to help you swallow more frequently.
————–
•From this point down, be careful because there are some strong drugs listed with some real potential side effects (and please remember, I’m not a physician giving out medical advice; I’m a basic scientist reading and writing about how one could possibly treat drooling). See your Movement Disorder Specialist, consult your personal Physician, and if possible/available, read through these cited review articles to help further educate you. Alternatively, consult the various Parkinson’s organizations: Parkinson’s Foundation drooling; Ask the MD: Potential Treatment for Drooling in Parkinson’s; Botulinum toxin (Botox) injections – can they help your symptoms of Parkinson’s disease?
•Oral anticholinergic drugs including Glycopyrrolate and Ipratropium bromide. Acetylcholine is the neurotransmitter used at neuromuscular junctions; thus, motor neurons release it to activate muscles. Acetylcholine is also a neurotransmitter in the autonomic nervous system (ANS). Substances that interfere with acetylcholine activity are called anticholinergics; they are potent drugs. Oral anticholinergic medications, as a class of drugs, generally reduce the production of saliva. Several have been tested for treating drooling in Parkinson’s. However, other side effects include mental difficulties, confusion, headache, dizziness, vomiting, drowsiness, blurred vision, constipation, and urinary retention. Be very careful if you use oral anticholinergics to treat drooling.
•1% atropine sulfate eye drops. Put 1 drop under the tongue 2-3 times/day to dry the mouth. Although atropine is an anticholinergic, it is thought that the local delivery reduces many of the systemic and potentially detrimental side effects.
•Activation of alpha-2 adrenergic receptors with Clonidine. Clonidine improved drooling in a randomized, double-blinded, placebo-control study in 32 drooling Parkinson’s patients.
•Botulinum toxin (Botox) A: Botox A is used to decrease saliva production. Direct injection of Botox A into the salivary glands reduces the amount of saliva produced. The most significant side effect from Botox A treatment is the thickening of oral mucous secretion.

The Continuation of the Story: To deal with my drooling, I’ve worked with a Speech-Language Pathologist, have done LSVT Loud, and recently started using Atropine sulfate (1 drop under my tongue about 2-3 times/day). Atropine starts to work almost immediately, and so far, there have been no side effects. For whatever reason, I’m balking at trying Botox A injections. I do have the name of an experienced ENT surgeon (Otolaryngologist), and this would be done in a clinic setting. I am also going to work to strengthen my swallowing muscles. The exercise goes like this: stick out your tongue slightly, and very gently bite down on it, and force yourself to swallow. Do 10 and then repeat the 10-swallows one more time. Try to perform this exercise a couple times per day. Good luck if you are also dealing with this nuisance of your Parkinson’s, rest assured you are not alone.
“Live neither in the past nor in the future, but let each day absorb all your interest, energy and enthusiasm. The best preparation for tomorrow is to live today superbly well.” Sir William Osler
Literature citations used in preparing this blog post:
Chou, K. L., Evatt, M., Hinson, V., & Kompoliti, K. (2007). Sialorrhea in Parkinson’s disease: a review. Movement Disorders, 22(16), 2306-2313.
Hockstein, N. G., Samadi, D. S., Gendron, K., & Handler, S. D. (2004). Sialorrhea: a management challenge. American family physician, 69(11).
Hyson, H. C., Johnson, A. M., & Jog, M. S. (2002). Sublingual atropine for sialorrhea secondary to parkinsonism: a pilot study. Movement disorders: official journal of the Movement Disorder Society, 17(6), 1318-1320.
Jost, W. H. (1999). Treatment of drooling in Parkinson’s disease with botulinum toxin. Movement disorders: official journal of the Movement Disorder Society, 14(6), 1057-1057.
Mier, R. J., Bachrach, S. J., Lakin, R. C., Barker, T., Childs, J., & Moran, M. (2000). Treatment of sialorrhea with glycopyrrolate: a double-blind, dose-ranging study. Archives of pediatrics & adolescent medicine, 154(12), 1214-1218.
Srivanitchapoom, P., Pandey, S., & Hallett, M. (2014). Drooling in Parkinson’s disease: a review. Parkinsonism & related disorders, 20(11), 1109-1118.
Tscheng, D. Z. (2002). Sialorrhea—therapeutic drug options. Annals of Pharmacotherapy, 36(11), 1785-1790.
Cover Photo Credit: https://www.pinterest.com/pin/212935888603784065/?lp=true

Thank you, Frank for yet another excellent article! My husband, Wyman, has been dealing with drooling this year and he did opt for the Botox. It has helped but takes several days to kick in & then stops working after about 6 weeks. We tried the pills-not good!!! Maybe the drops are in his future. Thank you again for the excellent explanation . Hope to see you at the PWR retreat. Kathay Smith
Sent from my iPhone
>
LikeLike
Thank you Kathay, I definitely appreciate your note and comments. I wish the best for Wyman and dealing with it b/c it is definitely a nuisance. Right now I’m scheduled to go to Tucson for a week for PT time; still trying to sort out whether or not I can I also go to the PWR! retreat. Frank
LikeLike
Hello Frank and Happy New Year! I really appreciate this post; as a social worker specializing in work with older adults, including those living with Parkinson’s, PSP, ALS, and other diseases that affect swallowing, I can really appreciate how sialorrhea can be a bothersome symptom. The physicians and nurses I work with often prescribe atropine drops, and I always make sure that I do an extra amount of education that even though the drug packaging says “opthalmic solution” and instructs application in the eye, the patient isn’t going to have much success treating sialorrhea if that’s where they put it 🙂
On a personal note, as I’ve gotten older I’ve found that swallowing pills has become more difficult (I used to be able to pop 3 ibuprofen without even a sip of liquid!), and I more frequently have food or drink “go down the wrong pipe,” resulting in coughing. While at this point a SLP would tell me not to worry about it, I’m aware that I may be at risk for dysphagia as the ole’ systems age, and I dread the idea of being stuck on a mechanical soft diet instead of all the crazy foods that I love to eat. I’m going to do your swallowing exercises along with you!
Love from DC,
K.t. Goettge
On Tue, Jan 22, 2019 at 11:02 PM Journey with Parkinson’s wrote:
> Frank Church posted: ” “The good physician treats the disease; the great > physician treats the patient who has the disease.” Sir William Osler “The > good physician treats the disease; the great physician treats the patient > who has the disease.” Sir William Osler “Listen to” >
LikeLike
Kate, happy new year! It’s so great to hear from you; I was telling someone recently about your time in the lab group. I’m glad you liked the post on swallowing issues in Parkinson’s, not a terribly exciting topic but important nonetheless. I need to go work on my lecture for this morning, will write again soon, take care of you, Frank
LikeLike