


“If you can’t explain it simply, you don’t understand it well enough.” Albert Einstein
“Be a voice not an echo.” Albert Einstein
Abstract: The VA Medical Center in Augusta, Georgia, reported the results of a six-month single-center, double-blind, placebo-controlled randomized study using Parkinson’s patients with early- and late-stage disease. They asked the question of whether low-dose daily niacin supplements could improve motor symptoms in Parkinson’s? This clinical trial assigned 21 of 47 patients to receive 250 mg niacin daily after a meal. Following the 6-months clinical study, all patients received niacin for an additional 6-months. The primary outcome measured was UPDRS III (Unified Parkinson’s Disease Rating Scale III); they also measured depression, sleep quality, cognition, and physical fatigue. Importantly, all but two patients tolerated the dose of niacin. The findings here indicate that daily treatment with low-dose niacin (250 mg/day) resulted in significantly improved motor function in Parkinson’s.
“The measure of intelligence is the ability to change.” Albert Einstein
Publication Details (Open Access, free to download, read, and print):
Wakade, C.; Chong, R.; Seamon, M.; Purohit, S.; Giri, B.; Morgan, J.C. Low-Dose Niacin Supplementation Improves Motor Function in US Veterans with Parkinson’s Disease: A Single-Center, Randomized, Placebo-Controlled Trial. Biomedicines 2021, 9, 1881. https://doi.org/10.3390/biomedicines9121881 (Click here access paper)
“You can’t use an old map to explore a new world.” Albert Einstein
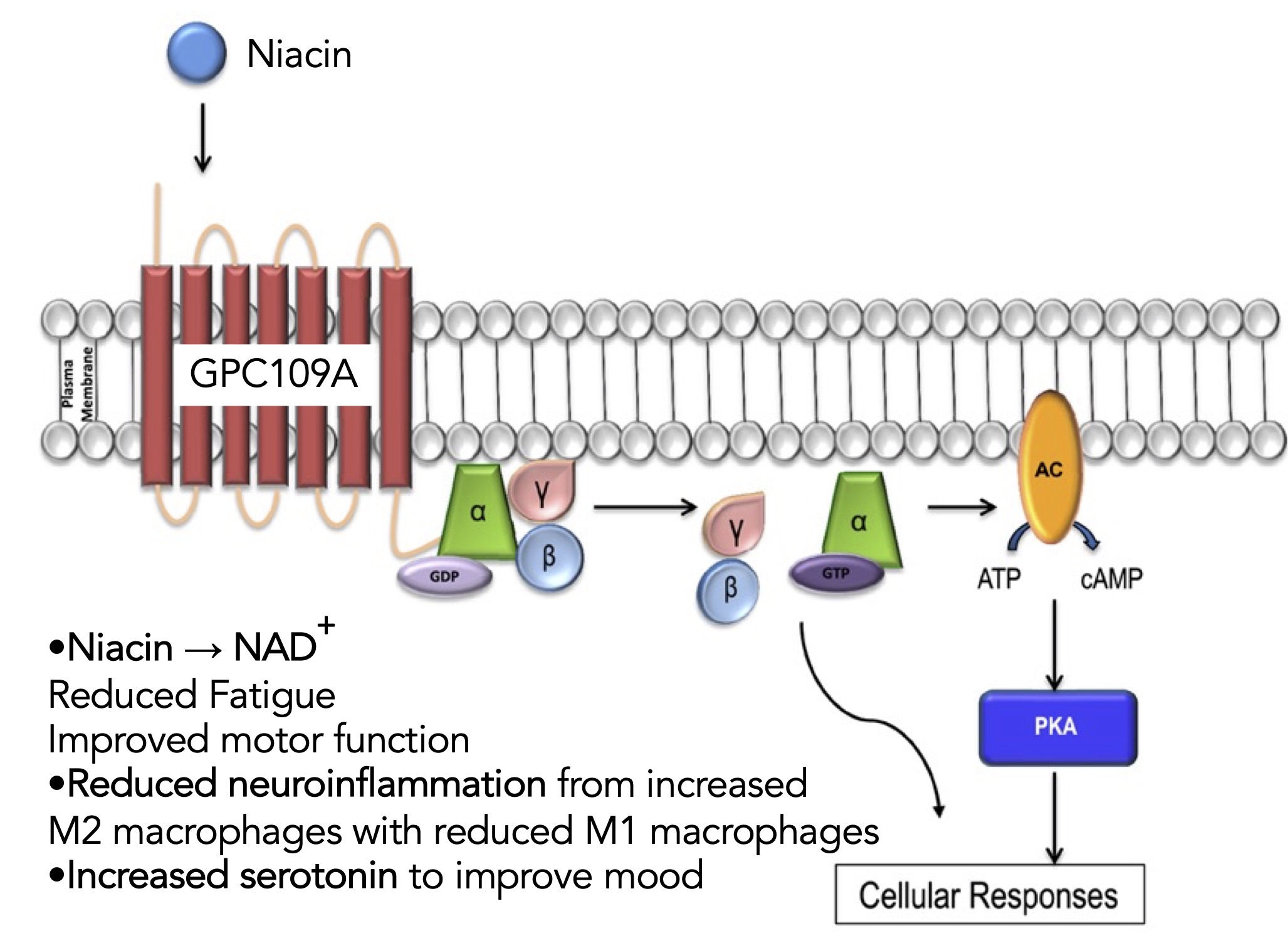
Putative Biological Mechanism Being Examined in this Clinical Trial with Niacin: Niacin binds to the niacin receptor on cells in the brain (a G-protein coupled receptor), presumably macrophages. Treatment with niacin is considered anti-inflammatory. Thus, it is thought that niacin upregulates M2 anti-inflammatory macrophages and reduces pro-inflammatory M1 macrophages. This fundamentally assumes the primary process to promote Parkinson’s is neuroinflammation. Then an anti-inflammatory response to negate this neuroinflammation is a reasonable hypothesis. See the figure below to explain their story (it is patterned after the graphical abstract presented by the authors).
“Failure is success in progress” Albert Einstein
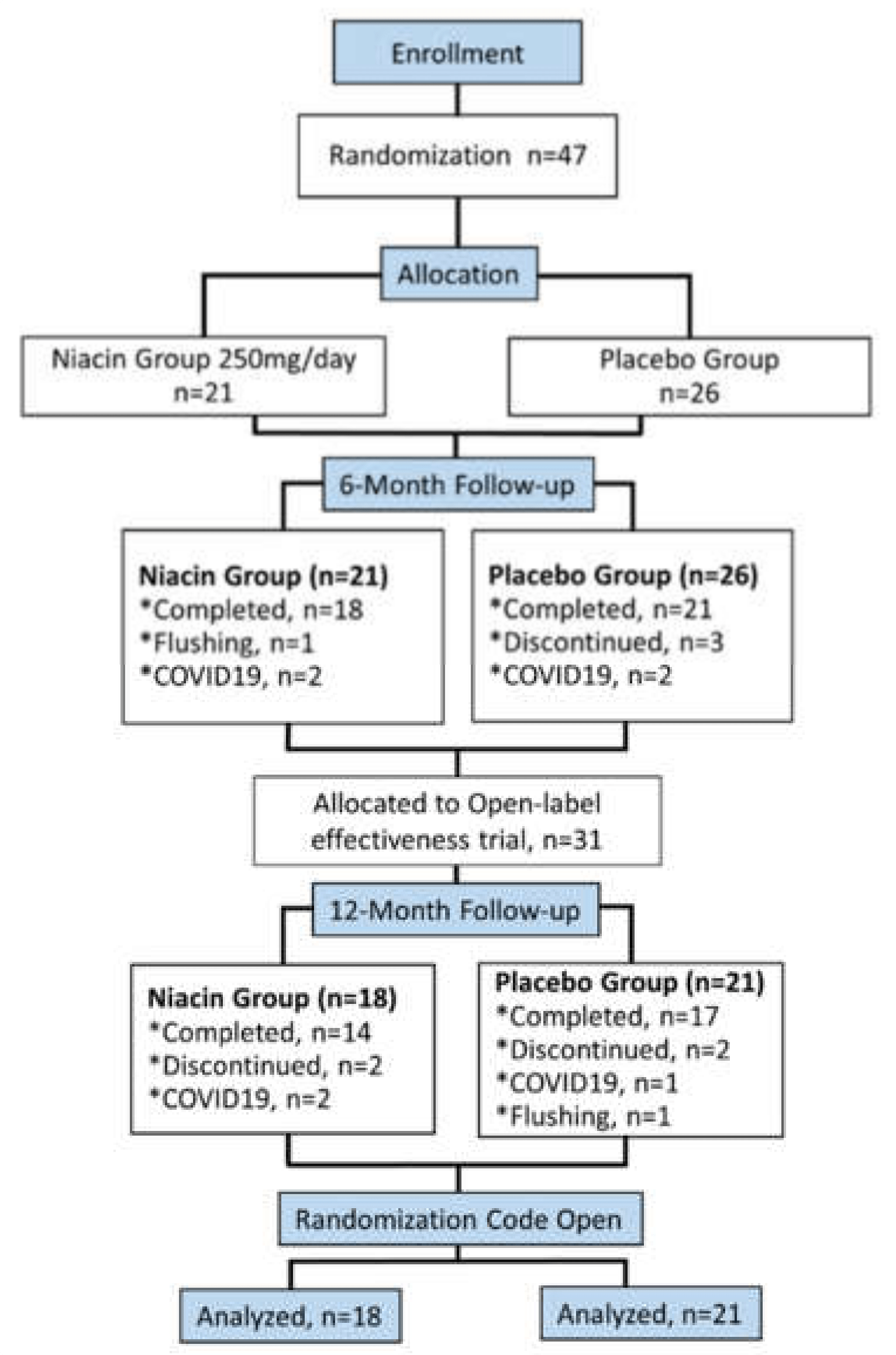
Study Description: Following the scheme detailed in the figure below, the trial began with 47 patients, and it finished with 39 patients (only two stopped due to flushing, others just discontinued, and several were dropped due to constraints of the COVID-19 pandemic). The flowchart shows randomly placed niacin (21 patients) and placebo (26 patients) at the end of 6 months, switched to open-label.
“If you want to live a happy life, tie it to a goal, not to people or objects.” Albert Einstein
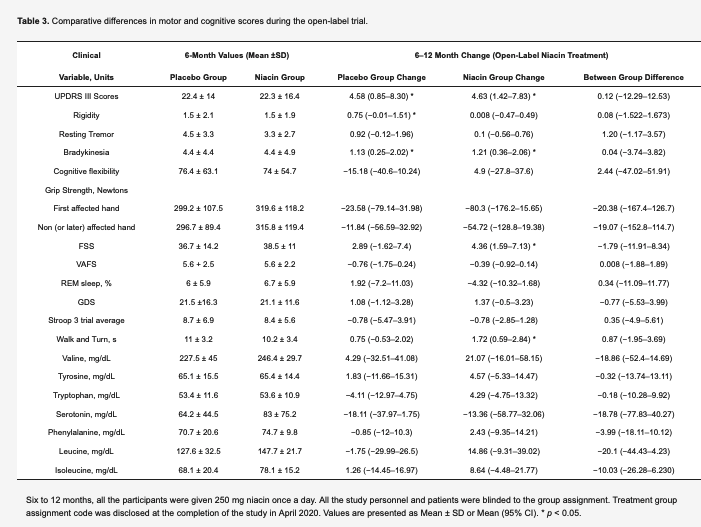
UPDRS III Scores from 6 to 12 Months of 250 mg Niacin daily: In the placebo group (now receiving niacin), the mean UPDRS III Scores were significantly decreased, as were the niacin group continuing their daily treatment (see Table below). Depending on the test group, they measured changes in bradykinesia, rigidity, and resting tremor, but not in all groups.
“Once you stop learning, you start dying” Albert Einstein
Secondary Outcomes: Grip-strength showed an increase in the niacin group but not the placebo. REM Sleep changed with the placebo but not the niacin group. Sleep efficiency (light, deep, or awake time) did not significantly change.
“Thinking is hard work; that’s why so few do it.” Albert Einstein
Strengths/Weaknesses to the Study:
- A well-designed study that showed a single daily dose of niacin (250 mg) in early- and late-stage Parkinson’s improved the overall UPDRS III scores, rigidity, and bradykinesia.
- The same person performed all the UPDRS III testing throughout the study.
- Their results show that niacin improved motor function and fatigue and stabilized serotonin and REM sleep percentages.
- Grip strength showed a trend increasing with niacin but was not statistically significant.
- The 250 mg daily dose of niacin produced negligible flushing when taken after meals, which was an instruction on how/when to take niacin.
- A limitation is the study size is relatively small, and the patient population tested was primarily older white men, with fewer women and minority populations.
- Another limitation is they did not directly measure levels of niacin.
- There was no measurement of neuroinflammation to determine the fundamental mechanistic role.
- A more significant and more prolonged clinical trial is now definitely warranted.
- However, the results presented suggest that low-dose niacin improves motor functions in Parkinson’s.
“In the middle of every difficulty lies opportunity.” Albert Einstein
Conclusions: This paper was just published earlier in December. I will consider adding it to my existing treatment regimen. However, I will bring it up with my Neurologist* first (by email at least). The Mayo Clinic lists a few warnings and precautions about taking niacin (click here to read it). Let me know if you are already using niacin or decide to add it to your daily take of substances for Parkinson’s.
Please Note: A follow-up blog post has been posted with some important information. This blog post can be read here (Click here).
*Medical Disclaimer: As with anything you read, please consult your Neurologist before taking niacin. While it appears totally safe, that does not mean it is right for you to take for your Parkinson’s.
“Live life to the fullest. You have to color outside the lines once in a while if you want to make your life a masterpiece. Laugh some every day. Keep growing, keep dreaming, keep following your heart. The important thing is not to stop questioning.” Albert Einstein
Cover Photo Image by David Mark from Pixabay

Hello, thanks for your very helpful post. My sister has PD and I am the care giver. What brand of Niacin do you take? I checked out Thorne Niacin but the dose is too high at 500 mg.
LikeLike
Philip, Amazon.com has the following product: NOW Supplements, Niacin (Vitamin B-3) 250 mg, Flush-Free, Nutritional Health, 180 Veg Capsules. They recommend taking 500 mg/day (2 capsules) but it would only take 1 capsule/day based on the paper. And the niacin is formulated in this product to release slowly and not cause the flushing issue. Hopefully, this will work well? But please talk to your sister’s Neurologist first, and Happy New Year! Frank
LikeLike
Thanks Frank. You are doing a great service to all PD patients by sharing your experiences. Much appreciated.
LikeLike
Thank you Frank. You are doing a great service to all PD patients by sharing your experiences. Much appreciated. Happy and Healthy New Year to you.
LikeLike
Thanks Frank for highlighting this research. Could you clear up a possible paradox. The researchers describe 250mg daily as low dosage whereas the Mayo link you thoughtfully provide suggests 11-18mg as the recommended daily intake. Is 250mg really low dosage or am I missing something
There are 2 issues here. The Mayo Clinic’s vitamin niacin need, suggests that one just need 11-18 mg/daily. Pharmacological use of niacin, starts at 250 mg and goes up to 3000 mg (or 3 gm/day). Dosing of 1 to 3 grams/day was shown to reduce serum LDL cholesterol and increase serum HDL cholesterol. Thus, based on this amount of niacin used in these cardiovascular clinical trials, the authors of the PD study saw that the majority of effect was in the low-dose range of 250 mg/day.
LikeLike
In fact there was an earlier 2018 study by the same authors on two doses of niacin for PD patients – 100 mg/day vs. 250 mg/day. Both doses showed efficacy in lowering neuroinflammation in PD patients. Interestingly, only patients in the 100 mg/day dose group reported improvement in quality of life compared to placebo. See https://doi.org/10.1016/j.jneuroim.2018.05.002
Higher doses of niacin, e.g. more than 1,000 mg per day, can result in higher fasting blood sugar. See https://pubmed.ncbi.nlm.nih.gov/11862304/
LikeLike
Philip, the group was starting another trial, I think at the lower dose (100 mg/day); however, COVID-19 and funding interfered and stopped their study. But it may be starting up again as we are emerging from the COVID-19-cloud to some extent.
Your comment is very interesting b/c using the lowest amount of drug would always seem to be the best route to follow, will definitely go read this article, thanks, Frank
LikeLike
I was actually a graduate student in the lab that performed these trials.
The first trial used100mg, 250mg, and placebo for 3 months. Which was extended to 1 year for everyone to take 250mg niacin. The effects at 3 months were not significant compared to the placebo, so a 6 month trial placebo vs 250mg was performed. The same issue occurred. Most data almost reached significance (serotonin levels significantly dropped in the placebo group, but not the niacin group. Many patients actually had unreadable serotonin levels when they started the study), but did not do so until the 1 year timepoint (but placebo comparison was only for the 6 months). Another trial began right before covid19, was paused and then restarted. This study was supposed to decrease the limitations from the previous trials. It was comparing niacin, niacinamide, and placebo for 18months, instead using two doses of 100mg daily (morning and evening doses). Unfortunately, recruitment was very low due to using the same VA, the pandemic, and the VA not allowing recruitment from other non-VA sites nearby (this was allowed in the previous study). Only seven patients were recruited during the available time (April 2020 and September 2020-March 2022). The next plan was to open it up to other VAs, but oversight above all VA research decided to shut it down because of the recruitment issue.
I was part of the lab for the 2nd and 3rd trials. They plan to submit some new grants within the next 6 months using the same protocol- niacin vs niacinamide vs placebo for 18months. This should elucidate the issue of the placebo effect (which is a substantial problem, particularly in PD patients who are very susceptible to the placebo effect). They plan to focus more on fatigue as it is one of the most common complaints of PD patients.
sidebar- the manuscript I was working on during my graduate career will be published soon with some very interesting data on the changes in blood biomarkers.
LikeLike
Thanks for that very detailed and interesting set of comments; I’ll be interested in seeing your paper when it comes out
and it is published, good luck, Frank
LikeLike
Hi Richard, Great point you make! It is considered low dose due to the fact that most pharmacological treatments with niacin use around 1g.
LikeLike
Thanks for the comment Marissa, that makes sense that the use of niacin here (250 mg) would be considered low dose, thanks! Frank
LikeLike
Richard, for most nutritional needs, we require very low doses of most vitamins, including niacin. When you get to higher doses of most compounds, then the over-the-counter phenomenon takes over, and taking higher doses ‘possibly’ brings on a therapeutic effect. However, this is not a recommended value for either niacin (250 mg / day as described in the article) or thiamine (3,000-4,000 mg / day as used by many daily for tremors and other issues in PD). Your second paragraph is a great explanation. Frank
LikeLike
I’m not sure if my comment was posted before or not. But that’s a great question, Richard! And you are absolutely correct. It is considered low-dose because most pharmacological interventions using niacin tend to use at least 500mg daily, which also increases the risk of side effects such as flushing and liver failure.
LikeLike
Another great answer
LikeLike