


“If you are always trying to be normal you will never know how amazing you can be.” Maya Angelou
“Hope and fear cannot occupy the same space. Invite one to stay.” Maya Angelou
Précis: This blog post’s primary goal is to present an overview of Carbidopa/Levodopa (originally named Sinemet) for treating Parkinson’s. A secondary objective was to describe the change in symptoms when my Carbidopa/Levodopa prescription was changed from Immediate-release (IR) to Controlled release (CR) tablets.
“Do the best you can until you know better. Then when you know better, do better.” Maya Angelou
Symptoms: When you have a disorder like Parkinson’s, you know your symptoms. You know them well. Last week I had a ‘rough’ time with my Parkinson’s; I was out of town for the week. When I got back home on Sunday night, I figured out the problem. My Carbidopa/Levodopa prescription was changed from the Immediate-Release (IR) to Controlled Release (CR) tablets. This was a whole new experience for me, re-experiencing my symptoms emerging after several years of what I would call a relatively stable life.
When I think about it, there are three strategies I follow for treating Parkinson’s. The first is traditional and deals with the “Cardinal Signs” (Symptoms), namely, tremor, stiffness, postural instability, and slowness of movement; these drugs are Carbidopa/Levodopa, and a dopamine agonist. The second type of compound, Complementary and Alternative (CAM), focuses on maintaining control of the brain micro-environment to keep the dopaminergic neurons left alive and functional. And the third class of medicine is the role of exercise to be neuroprotective and, hopefully, promote neuroplasticity.
“Continue. Be loving and be strong. Be fierce and be kind. And don’t give in and don’t give up.'” Maya Angelou
Brain Chemistry 101- the Physiology, Biochemistry, Neurobiology, and Pharmacology of Dopamine and Carbidopa/Levodopa: This is not a comprehensive review of everything related to dopamine and Carbidopa/Levodopa. I find it beneficial personally to make schematics/figures and use them to drive the narrative. Hopefully, this material is new information for some of you, and likely, it’s a review of information for others. Regardless, enjoy.
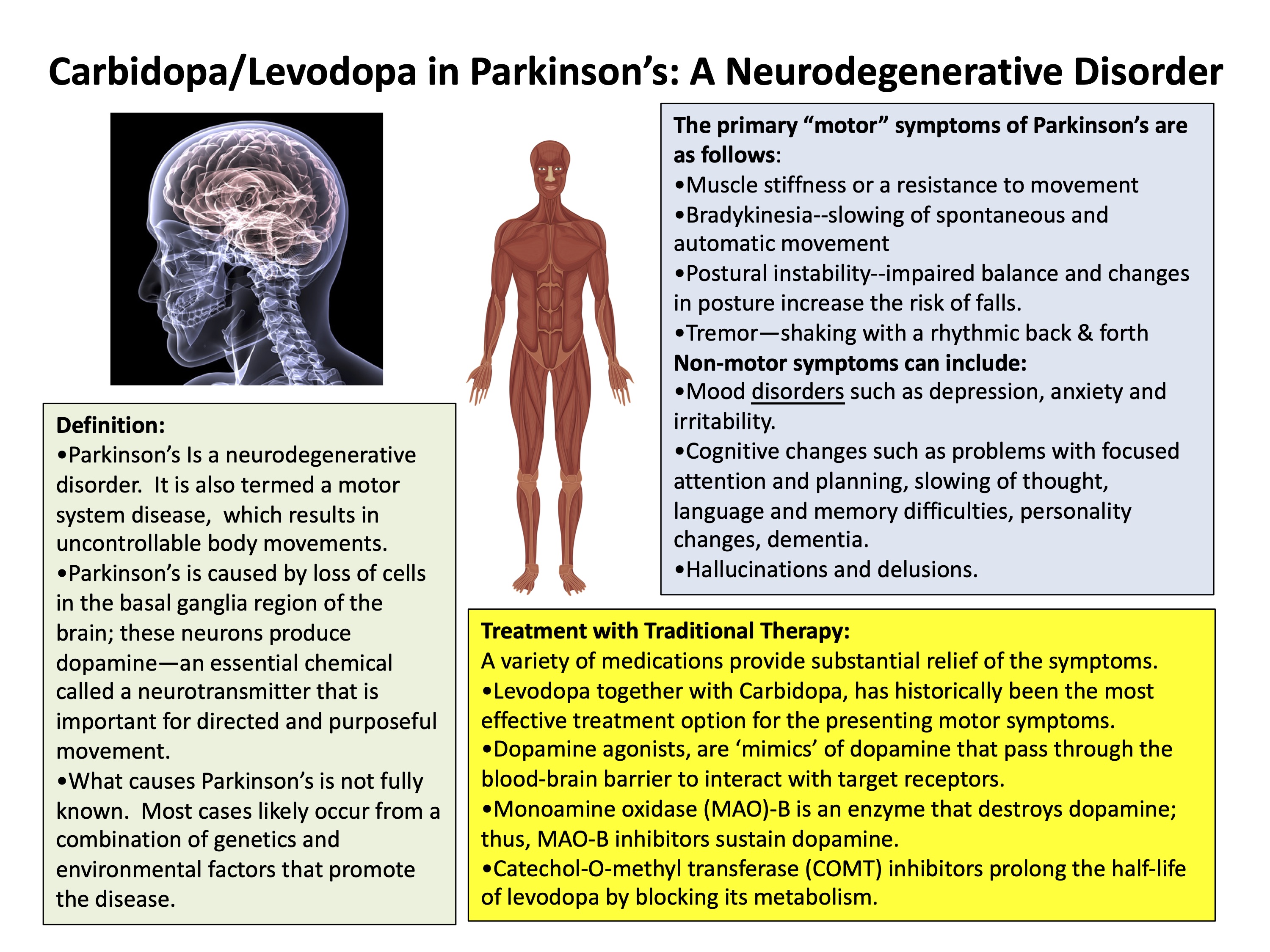
An Introduction to Parkinson’s: Included below is a one-page figure with a definition for Parkinson’s, the primary motor symptoms and non-motor symptoms for this disorder, and the most common treatment therapies using traditional pharmaceutical drugs.
“My mission in life is not merely to survive, but to thrive; and to do so with some passion, some compassion, some humor, and some style” Maya Angelou
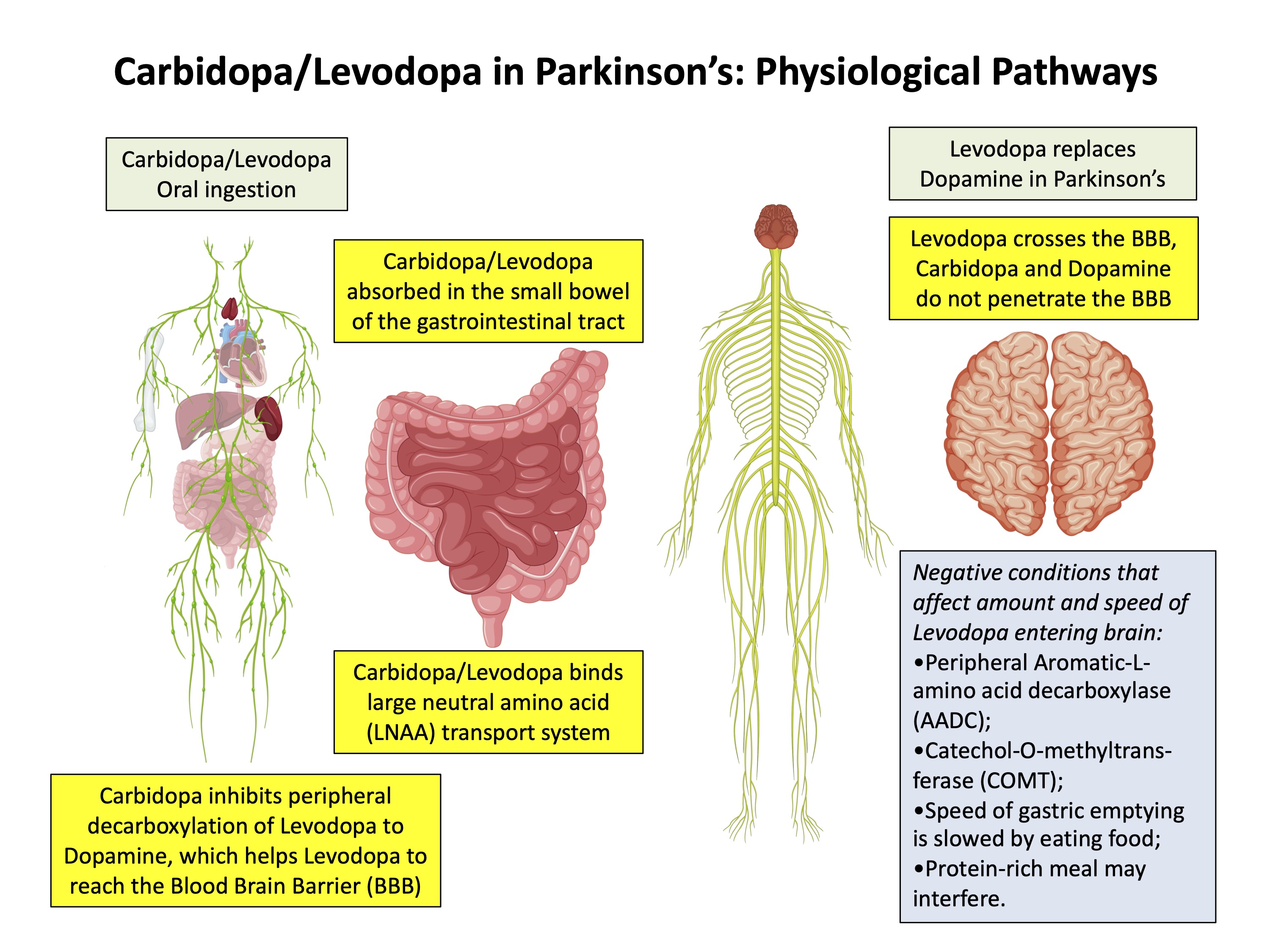
Carbidopa/Levodopa in Parkinson’s- Physiological pathways: Dopamine is known as a neurotransmitter, and it is found mostly in the central nervous system. Neurotransmitters are endogenous substances that transmit signals across a synapse from one neuron to another “target” neuron or another nerve fiber, a muscle fiber, or some other structure. There are no alternative pathways to synthesize dopamine, so people-with-Parkinson’s make less of it; therein lies the beginning of Parkinson’s.
Carbidopa/Levodopa is the gold standard for treating Parkinson’s. As shown in figure 2, most of us will ingest it orally, and the Carbidopa/Levodopa will be reabsorbed in the lower part of the G.I. tract and taken up by the large neutral amino acid transport system. Carbidopa is essential because it prevents Levodopa’s activation before it reaches the blood-brain barrier. This inappropriate dopamine activation would give all sorts of harmful side effects to having dopamine activated peripherally. Two naturally occurring enzymes have levodopa as their substrate, peripheral aromatic-L-amino acid decarboxylase and catechol-O-methyltransferase. Next, it is also vital to realize Levodopa is an amino acid type structure and is taken up by amino acid transport systems (reminder: proteins are composed of amino acids) Therefore, a protein-rich meal could interfere with the uptake of the Carbidopa/Levodopa. However, there have been several publications that have refuted this exact notion. Nonetheless, it’s probably best to take Carbidopa/Levodopa on an empty stomach.
“Success is loving life and daring to live it.” Maya Angelou
Carbidopa/Levodopa in Parkinson’s- Biochemistry: The amino acid tyrosine, usually derived from dietary proteins, enters the brain in the circulating blood. Tyrosine is taken up into neurons by amino acid transporters in the brain. The enzyme tyrosine hydroxylase catalyzes the conversion of tyrosine to dihydroxyphenylalanine (L-DOPA). L-DOPA is converted to dopamine by the enzyme aromatic-L-amino acid decarboxylase (it is also called L-DOPA decarboxylase). This enzyme so quickly changes L-DOPA to dopamine, that supplying the enzyme with additional substrate (L-DOPA) leads to increased product formation (dopamine), which is the basis of L-DOPA (or Levodopa) treatment for Parkinson’s.
When you’re talking about it from a pharmaceutical standpoint as a drug, Levodopa is the same thing as L-DOPA. What’s interesting about this organ is the route compounds enter the brain through the blood-brain barrier. It says that the brain actively controls with the blood-brain barrier what is allowed to enter into the brain. See Figure 3 for more details amid biochemical reactions of tyrosine, L-DOPA (Levodopa), Carbidopa, and dopamine.

“If you must look back, do so forgivingly. If you will look forward, do so prayerfully. But the wisest course would be to be present in the present gratefully.” Maya Angelou
Carbidopa/Levodopa in Parkinson’s- Synthesis of dopamine: In 1958, the Swedish scientists Arvid Carlsson and Nils-Åke Hillarp, discovered the function of dopamine as a neurotransmitter. Dopamine has diverse actions that include motor control, cognition, emotion, motivation, reward, reinforcement, and neuroendocrine and cardiovascular regulation. The figure below shows the substrates and enzymes that generate dopamine, which is then released by a neuron to signal the receiving cell after binding to dopamine receptors. Dopaminergic neurons are found in three major regions: (i) substantia nigra neurons that mainly serve the putamen and the caudate nucleus; (ii) dopaminergic neurons in the ventral tegmental area and preferentially innervate the ventral striatum and the prefrontal cortex; and (iii) dopaminergic neurons are located in the arcuate nucleus of the hypothalamus. There are two major classes for five dopamine receptors, namely, D1-like receptors (D1A–1D and D5) and D2-like receptors (D2, D3, and D4). Activation of D1-like receptors results in the generation of adenylyl cyclase, which gives you more cAMP. By contrast, activation of D2-like receptors blocks the formation of cAMP by inhibiting adenylyl cyclase.

“A joyful spirit is evidence of a grateful heart.” Maya Angelou
Carbidopa/Levodopa in Parkinson’s- Combining Levodopa with Other Substances Changes Its Properties: Many drugs contain Levodopa (= L-DOPA) as their primary active ingredient, including Sinemet, Stalevo, Madopar, and many others. I presented the ‘big-picture’ of making dopamine and using Levodopa in Parkinson’s. Also discussed was the use of Carbidopa to allow the Levodopa to go from the gut to the circulatory system to get to the blood-brain barrier. Many questions remain, consider the following: why do we take Levodopa so frequently? Can you make Levodopa last longer?
Why do we take Levodopa so frequently? Every compound or drug has a real-time half-life. Basically, how long does a drug last in the body or bloodstream. Some are long-lived, some are very short, and Levodopa falls in the category of relatively short half-life (it is about 1 hr), so at 60 min 50% is gone, at 120 min 75% has been consumed, and 6.25% remains after 4 hours. This loss of drug assumes no other factors are contributing to alter the drug’s half-life. Importantly, Carbidopa increases the half-life of Levodopa to ~90 min.
With such a half-life, could you take Carbidopa/Levodopa more frequently to maintain an equivalent dose? For example, let’s say you take six 25 mg Carbidopa/100 mg Levodopa IR tablets per day (you take two tablets three times per day at 6 AM, noon, 6 PM). Instead, could you take one tablet every 3 hours (6 AM, 9 AM, noon, 3 PM, 6 PM, 9 PM)? A total disruption to your daily activity taking tablets all day long, but would this dosing strategy give you a more consistent way to deal with any off-on fluctuation? Or would the level reached by one tablet, compared to two tablets, just not be sufficient? (NOTE: this is a Biochemist thinking out loud, definitely consult with your Neurologist before considering or even trying such a strategy!).
Can Levodopa be made to last longer? We already do this by adding it with Carbidopa, which is in Sinemet and Stalevo. Madopar tablets contain Levodopa and Benserazide instead of Carbidopa to inactivate peripheral aromatic-L-amino acid decarboxylase. Others take compounds that directly change dopamine’s availability; many of you are taking a monoamine oxidase B inhibitor, either Selegiline or Rasalagine (Azilect). Stalevo is a drug consisting of Levodopa, carbidopa, and entacapone, which in an catechol-O- methyltransferase (COMT) inhibitor.
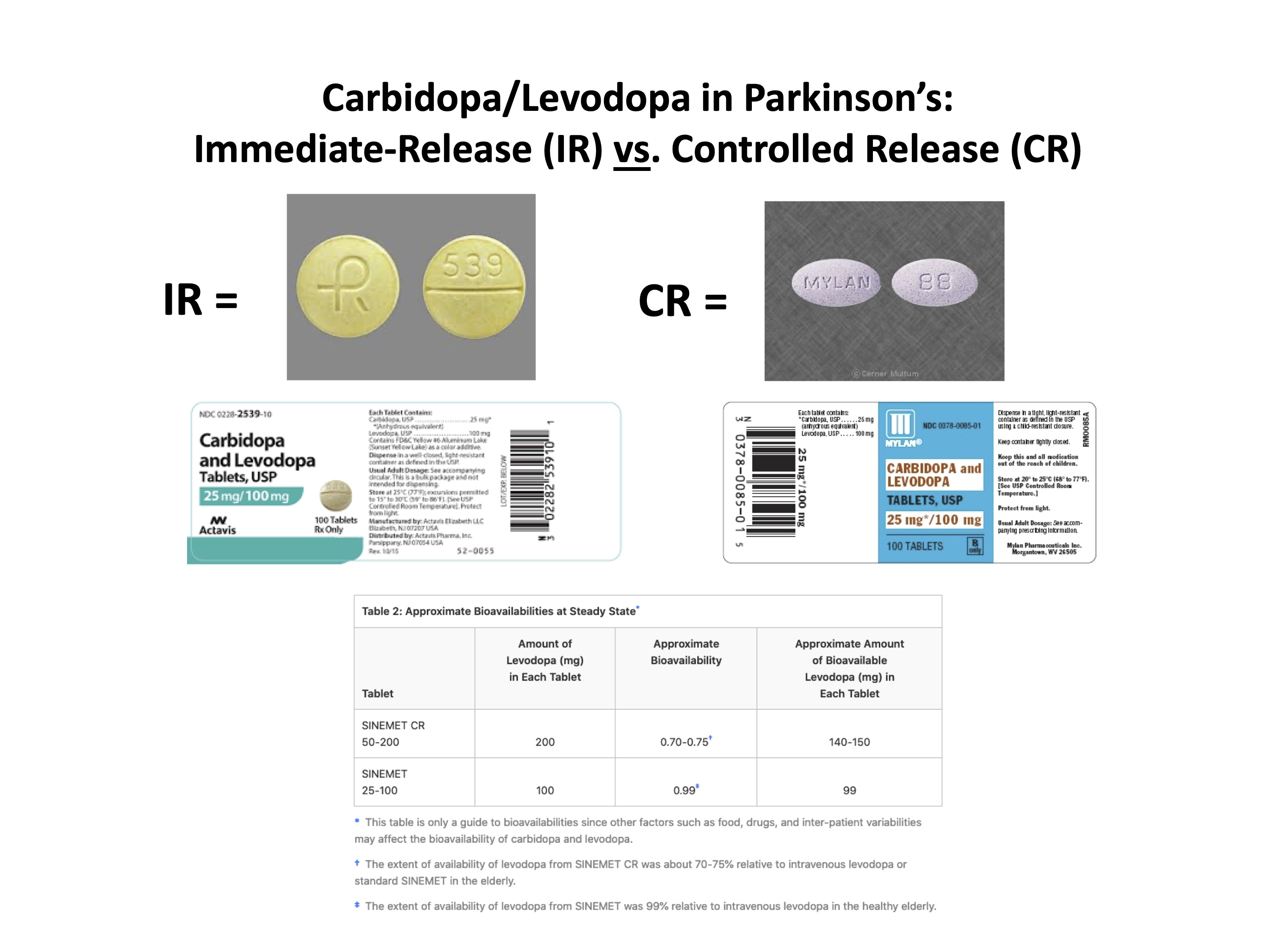
Another way is to have the Levodopa released in a timed- or controlled-based manner, which is the critical feature of Sinemet CR (controlled release) tablets. However, from the literature, several Sinemet CR features are not ideal for many people. There is less available drug per pill; it takes longer to ‘kick-in’; however, for others, this regularity is a key to monitoring your ‘off-on’ periods. And one compound, Rytary, basically has an extended-release formula for Levodopa. The two figures below give an overview of Levodopa’s various forms and how it yields different response times.

“When you learn, teach, when you get, give.” Maya Angelou
My Misadventure Taking Caribodpa/Levodopa CR Instead of Carbidopa/Levodopa IR: I feel that we have a delicate balance between the consumption of available dopamine we make each day and its replacement through Levodopa or CAM means. For me, I disrupt the balance by stress, over-work, too little sleep, strenuous exercise, and some other scenarios, but you get the picture? I think we are usually right at the appropriate level of dopamine (as good as it’s going to get with Parkinson’s), where a change in physiology or medication could negatively alter the way your move, feel, and act. I also think over time, we can sense these changes in our bodies, e.g., you forget to take your Carbidopa/Levodopa, and you go 12 hours, not 6 hours, between pills- you feel the change.
I was recently (and inadvertently) switched from Carbidopa/Levodopa IR to Carbidopa/ Levodopa CR. I was out of town, and I took Carbidopa/Levodopa CR for a week before realizing that I was having motor problems, and the only change I had made was this ‘different’ Levodopa compound. Susan started asking me, “How was I feeling?” She could tell something was ‘off’ in me. Briefly, I was stiffer, less mobile, less stable; my voice was weaker, my posture was worse, I felt more vulnerable, and my thought process seemed less clear. All the symptoms I had felt a couple of years ago had started coming back in a couple of days. Remember, we measure the ‘progression’ of Parkinson’s over months-to-years, not days.
According to the literature, the bioavailability of Carbidopa/Levodopa CR is ~70% compared to Carbidopa/Levodopa IR. Time to action is prolonged (I could feel the CR working somewhat in about three hours, whereas the IR, I can tell, is working in about 45 minutes). It was my fault for not thinking something was going on with the drug earlier in the week. I could have taken Carbidopa/Levodopa CR more frequently (gone from 6 to 4 hrs) or increased my dose; however, I do not enjoy being a neurologist. When I got home, I realized the problem. Re-started Carbidopa/Levodopa IR, and in five days, I was back to where I thought was my ‘old-normal-self’ in the occupancy of Parkinson’s. I had disrupted my daily balance of dopamine by taking the ‘different’ Carbidopa/Levodopa. And it all made sense when you consider the half-life of Levodopa, reduced bioavailability of Carbidopa/Levodopa CR coupled with the schedule and the amount I was taking, and the delicate daily need between synthesis-consumption of dopamine. To add fuel to the fire, I usually take 1/2 of a tablet twice/day; afterward, from reading the insert for the Carbidopa/Levodopa CR it says not to break them up (presumably further reduces bioavailability).
If you feel different from taking your drugs, the moral of the story, and you feel worse, get in touch with your Neurologist and take action. We all react differently to these drugs, such is our disorder with Parkinson’s. I am not criticizing Carbidopa/Levodopa CR; it is the preferred drug for many people. It just did not work for me. And I learned a valuable lesson.
“You may not control all the events that happen to you, but you can decide not to be reduced by them. Try to be a rainbow in someone else’s cloud. Do not complain. Make every effort to change things you do not like. If you cannot make a change, change the way you have been thinking. You might find a new solution.” Maya Angelou
Cover Photo Image by Kohji Asakawa from Pixabay

Thanks for writing this Frank. It was very informative to me.
Mike, thanks for the note, glad it was helpful. Best wishes, Frank
LikeLiked by 1 person
Hi Frank,
Thanks for sharing this experience. I’m wondering how you identified the difference between the IR & CR tablets. I assume there was a physical difference (pill shape and/or number), bur perhaps there was not? I ask because I have had strange, but sporadic experiences in recent months that matched your description. Times that felt like a dose was “missed” only to mysteriously kick in between 2 hours and 45 minutes to 3 hours later (instead of my usual 55 minutes).
I have both IR and ER prescriptions (ER at night to help sleep), and the pills are very different…I’d never get them confused. But your post has me wondering if there is some mixup in my IR tablets…they’re generic, and I get 3 months supply at a time. The pill shape and number are clearly IR, but could a generic manufacturer make this mistake.
LikeLike
Brett, a picture of the tablets is given in the figure in the blog post, round yellow for the IR tablets, and the CR tablets are green and oblong. I knew they were different generics, I just didn’t see the CR on the label, or failed to look closely. Here’s what we should all realize is the FDA allows companies a leeway of 20% difference from the parent drug. I have read a lot of complaints from other PwP about the differences between the various generics carbidopa/levodopa drugs compared to the original Sinemet. My IR tablets have been supplied by Actavis and I have used this specific generic for Sinemet for several years. I really don’t have a good answer to your question. I am absolutely convinced now that the pharmacy made a mistake by ordering the CR instead of the IR, they finally acknowledged the order mistake. Thus, the ‘effect’ I exhibited that week was clearly aligned with taking the CR in place of the IR. Your timing mentioned above is essentially the same timetable I found for the CR vs IR;; however, from your question, I just don’t know if that big of a difference could exist ‘within’ a given IR tablet. Frank
LikeLike
As always you provide much needed education in a manner that understandable and very relevant !, Thank you Frank
LikeLike
Thanks Drew, I really enjoyed writing this post. And I think we’ve all had some occasional ’strange’ problems with drug therapy for PD. It was relevant for me to describe it; the overview and educational parts were really fun to write. thanks again, Frank
LikeLike