


“Patience and fortitude conquer all things.” Ralph Waldo Emerson
“I know of no higher fortitude than stubborness in the face of overwhelming odds.” Louis Nizer
Overview: Recently, I reviewed a clinical trial involving ablation of the globus pallidus by focused ultrasound to treat Parkinson’s (click here to read this blog post). Some time ago, I was asked my opinion about using Focused Ultrasound Ablation (FUSA) on the pallidothalamic tract (PTT). Herein is an overview of FUSA-PTT.
“It is by surmounting difficulties, not by sinking under them that we discover our fortitude.” Hannah Webster Foster
Rationale: The FDA (in the USA) has approved the use of FUSA for treating tremor-dominant forms of Parkinson’s that have a therapeutic point of poorly responding to current therapy. A group of Neurologists genuinely believe that focused ultrasound can be used to achieve symptomatic relief of motor symptoms by ablating elements of the basal ganglia.
There is a long history of ablative neurosurgery on various basal ganglia regions. The basal ganglia can be considered the brain’s central processing unit for receiving, organizing, and implementing motor functions. The idea may sound somewhat brutal by ablating brain tissue, but chronic therapy-resistant Parkinson’s provides only a few options. Deep brain stimulation (DBS) surgery and FUSA are considered viable options.
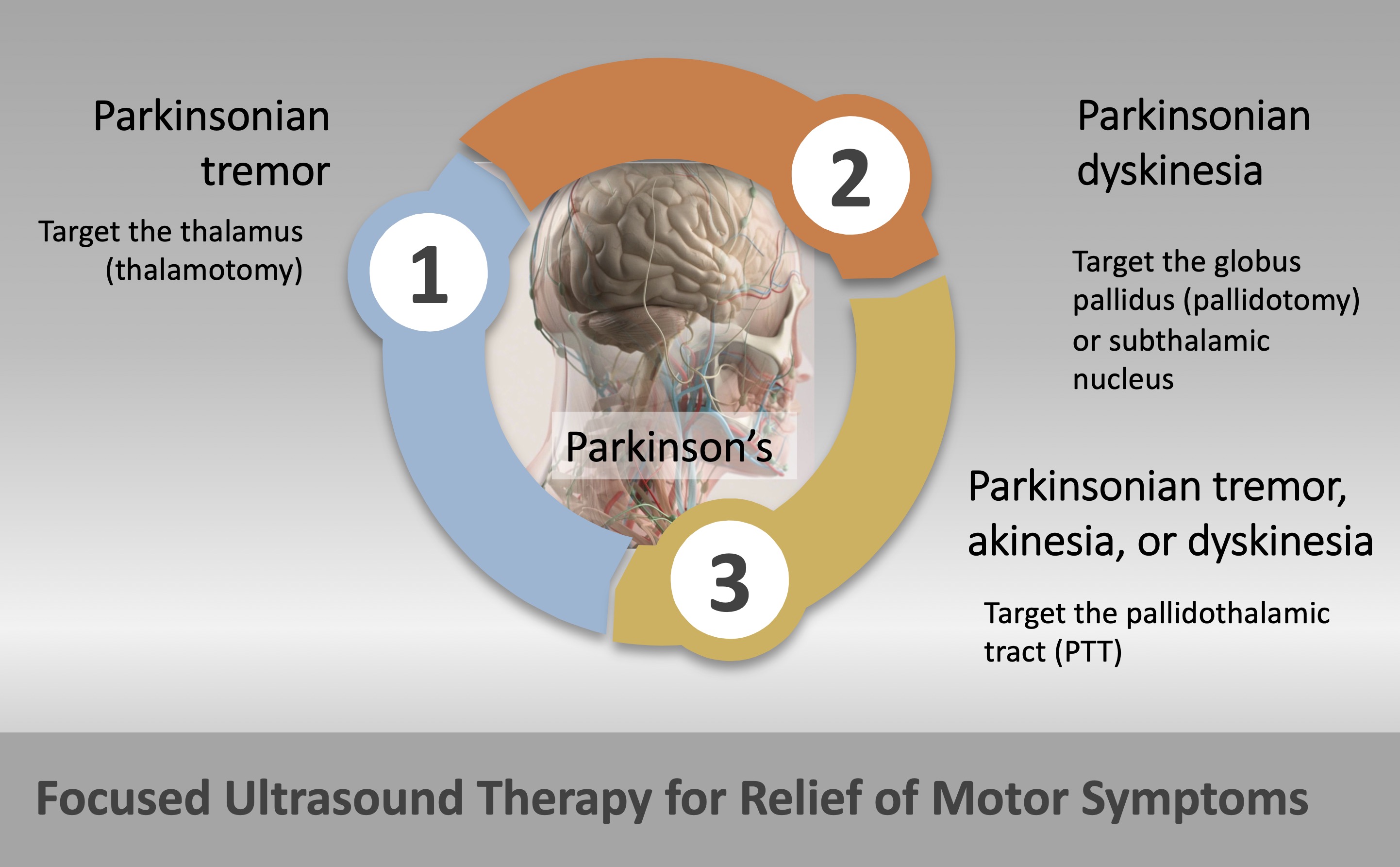
The symptoms that can be relieved by FUSA are summarized in the following drawing by using focused ultrasound to ablate part of the basal ganglia:
A Simple Analogy: While it may only be early March, the past two weeks have seen temperatures average in the upper 70s-low 80s (oF), and the central air conditioner (A/C) has been needed (mainly for reducing the humidity in the house). Until yesterday, it stopped altogether. At eleven years old, we hoped it last a few more years. The A/C repair person assessed the problem. Two solenoids in the outside cooling unit receive signals from the furnace and thermostat in the house. They were over-active, and bypassing them from the system restored cool air into the home. My simple A/C analogy has these hyperactive solenoids in the cooling unit represented by the thalamus, globus palllidus, subthalamic nucleus, or pallidothalamic tract. The A/C technician removing the hyperactive solenoids is like the neurosurgeon ablating brain tissue using focused ultrasound.
A feeble analogy, especially since my entire understanding of electrical circuits was in a college Physics Laboratory course. Hopefully, the metaphor of faulty solenoids being bypassed from the system to restore A/C airflow is vaguely similar to FUSA to ablate brain tissue to restore more normal-like motor function in Parkinson’s. Like in my A/C story above, bypassing the solenoids refreshes cool air, but the defect remains in the system. Likewise, ablating brain tissue by FUSA does not get to the cause of Parkinson’s. Instead, it reroutes disruptive signals to hopefully alleviate and restore a defective motor pathway.
A Conduit Named Pallidothalamic Tract (PTT): The PTT connects the globus pallidus internus and the ventrolateral portion of the thalamus. Ablation of the PTT is thought to be anti-Parkinson’s, especially relevant in chronic therapy-resistant Parkinson’s. The pioneers of the PTT reside in Switzerland. Aufenberg et al. (2005) and Magara et al. (2014) showed that focused ultrasound ablation of the PTT significantly improved tremors, dyskinesia, and akinesia. Furthermore, these patients had reduced levodopa equivalent daily dose (LEDD). More recently, Gallay et al. (2020) reported the results of fifty-one chronic-therapy-resistant Parkinson’s patients by FUSA of the PTT. The patients had an 88% mean tremor relief and 82% mean global symptom relief on the operated side, and 69% mean global improvement in the whole body.
Aufenberg, Christoph, Johannes Sarnthein, Anne Morel, Valentin Rousson, Marc Gallay, and Daniel Jeanmonod. “A revival of Spiegel’s campotomy: long term results of the stereotactic pallidothalamic tractotomy against the parkinsonian thalamocortical dysrhythmia.” Thalamus & Related Systems 3, no. 2 (2005): 121-132.
Magara, Anouk, Robert Bühler, David Moser, Milek Kowalski, Payam Pourtehrani, and Daniel Jeanmonod. “First experience with MR-guided focused ultrasound in the treatment of Parkinson’s disease.” Journal of therapeutic ultrasound 2, no. 1 (2014): 1-8.
Gallay, Marc N., David Moser, Franziska Rossi, Anouk E. Magara, Maja Strasser, Robert Bühler, Milek Kowalski et al. “MRgFUS pallidothalamic tractotomy for chronic therapy-resistant Parkinson’s disease in 51 consecutive patients: single center experience.” Frontiers in surgery (2020): 76.
One or Two? In the USA, focused ultrasound is approved to treat only one side of the brain; thus, the impact of surgery will affect only one side of the body. However, clinical trials are underway to treat patients on both sides of the brain (bilaterally). Several clinical trials are underway in the USA, Japan, and Europe to study the feasibility and safety of focused ultrasound to treat different symptoms of Parkinson’s. Some of these clinical trials will assess the FUSA of the PTT by comparing unilateral to bilateral pallidothalamic tractotomy.
In 2021, Gallay et al. reported a study with ten patients of bilateral FUSA of the PTT. They followed these patients for a year after receiving the second PTT. This is an interesting paper with an honest assessment of what worked and what did not work in these patients. I encourage you to read it thoroughly if you are interested in exploring FUSA-PTT for the treatment of chronic therapy-resistant Parkinson’s.
They start by stating that to justify brain surgery, in the framework of a lesioning procedure, this intervention should provide globally better results than drug therapy. Keep this point in mind. One year after bilateral PTT, the patients reported a high global symptom relief for both sides of the body. However, they found that axial symptoms were the most difficult to control. Axial symptoms are summarized in the drawing below (click here to read more from the source).
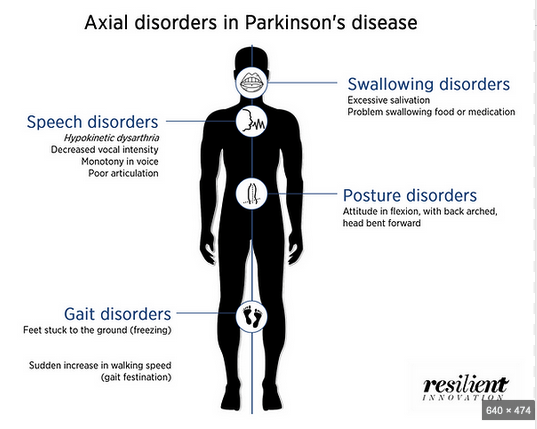
This study found that scoring for axial items, gait, and postural instability remained unchanged after 1-year bilateral FUSA of the PTT. Furthermore, scoring revealed a 58% worsening of speech [hypophonia (reduced speech intensity), tachyphemia (rapid speech, often having erratic rhythm and grammar and mixed with irrelevant words), and reduced speech initiation].
Please remember that this procedure does not alter disease progression; thus, one speculative conclusion is the possibility of disease progression unimpeded by the FUSA-PTT process. I like the following statement, and I want to quote the paper: “Gait is the key to independence and voice to communication, two essential psychosocial components of human life. The strength of the neurodegeneration concept imposed on PD patients and threatening their bodily and mental functions cannot be underrated. It can explain the modest improvements of emotionality and quality of life described by our patients in spite of very significant and multiple symptom reductions.” They concluded that a more extensive series of patient evaluations are needed to advance their hypothesis about FUSA of the PTT.
Gallay, Marc N., David Moser, Anouk E. Magara, Fabio Haufler, and Daniel Jeanmonod. “Bilateral MR-guided focused ultrasound pallidothalamic tractotomy for Parkinson’s disease with 1-year follow-up.” Frontiers in neurology (2021): 20.
The Next Step and Concluding Comments: As a biological chemist and person-with-Parkinson’s, I greatly ponder our situation and think about others further along in their disease progression.
It scares me to think I may need DBS or FUSA at some point in time when my medications have failed me. These last two blog posts make me pause and consider the future.
My calcitrant mind tells me to double my daily workout and start doing much more aerobic exercise (I remember those lab mouse studies where the rodents ‘ran off’ their chemically-induced Parkinson’s on a running wheel).
Alternatively, my even-keel mode tells me that over time, these surgical techniques (DBS vs. FUSA) will come full circle, and we will have a better choice of options for treating chronic therapy-resistant Parkinson’s.
My science-minded part has not given up on the brilliant group of folks studying the pathophysiology and signaling pathways that could one day lead to better therapeutic drugs to treat Parkinson’s.
And my enthusiastic mind still wants to remain positive and reinforce the current options and, hopefully, the new options coming soon.
In closing, I will continue to read and educate myself (and us) about the various options available as we approach chronic therapy-resistant Parkinson’s. Please remain active, hopeful, optimistic, persistent, and informed regardless of our current or future situation. As always, you are still you.
“The king-becoming graces,
As justice, verity, temp’rance, stableness,
Bounty, perseverance, mercy, lowliness,
Devotion, patience, courage, fortitude,
I have no relish of them, but abound
In the division of each several crime,
Acting in many ways.” William Shakespeare

Thanks Frank for the excellent article . This was such a great analysis and very informative for me and I will refer back to this often
LikeLike
You are most welcome.
LikeLike
Isn’t what MJ Fox had done the open surgery method of pallido-thalimotomy FUS?
LikeLike
I really do not know the answer to your question. Sorry, Frank
LikeLike
.Frank, thank you for the excellent overview. Let me share my personal experiences regarding ptt qblation clinical trial since I am a participant. First a little critic: you are assuming that the procedure done in Switzerland and the one done in the US clinical trials are the same. I would say that at best we don’t have enough information for such conclusion. For that matter when the Swiss team found out about the US clinical trials they took the trouble to publish a disclaimer statement in the Neurosurgery stating that nobody from US contacted them regarding this procedure and they don’t have any knowledge about the clinical trials. This was authored by Mr Moser. I specifically asked the surgeon if it was an identical target and he stated that
At in general it was the same target but the procedure wasn’t the same. I have to tell you that I went through the evaluation process at the Swiss clinic and I was told that I would not be a good candidate for this procedure. Wheen I went through the evaluation in US I was told that I would be an excellent candidate for the surgery.. Well I will tell you what happened tomorrow since it’s getting late. Frank, thank you for the excellent overview. Let me share my personal experiences regarding ptt qblation clinical trial since I am a participant. First a little critic: you are assuming that the procedure done in Switzerland and the one done in the US clinical trials are the same. I would say that at best we don’t have enough information for such conclusion. For that matter when the Swiss team found out about the US clinical trials they took the trouble to publish a disclaimer statement in the Neurosurgery stating that nobody from US contacted them regarding this procedure and they don’t have any knowledge about the clinical trials. This was authored by Mr Moser. I specifically asked the surgeon if it was an identical target and he stated that
At in general it was the same target but the procedure wasn’t the same. I have to tell you that I went through the evaluation process at the Swiss clinic and I was told that I would not be a good candidate for this procedure. Wheen I went through the evaluation in US I was told that I would be an excellent candidate for the surgery.. Well I will tell you what happened tomorrow since it’s getting late.
LikeLike
Hi, this is continuing comments about my experience participating in the clinical trial . I have to tell you that after the first procedure I felt considerably better. Not right away. After several weeks of intense physical therapy I was free of dystonia and dyskinesia. I could take the ldopa 4 times a day (Rytary 195mg 2 pills) and I felt very slight dyskinesia on untreated side which was my indication that the medication was working and I was on. Before the procedure I had terrible off periods and I was very sensitive to animal protein. After the procedure I felt that my off periods were much better than before and I was not as sensitive to the animal protein. Overall I felt much better about 9months after the first procedure. I had to make a decision whether to go for the treatment u of the second side or to keep 1l side treated. . My worry was the possibility of the disease switch to the unt=eaten sidend outside of the clinical trial I would be in quite a predicament. I consulted with the neurosurgeon who did the first treatment and he definitely recommended to go with the second side ablation. I did that and I regret that decision. I am 9 months past the procedure and I am not anywhere close to the 1st post treatment status. One of the biggest problems is the fact that I am not as sensitive to the ldopa. I also developed every symptom you describe here ( or more accurately dr Galloway indicated ). Iam working with the physical therapist trying to resolve these new issues but I am not optimistic that I will be at that level.
LikeLike
Felix, thank you for the detailed description of your procedure and the response to your body. Wow, you have been through a lot and hopefully, your work with the PTs will improve your symptoms. Since I am not a neurosurgeon, I am confused about why surgical approaches would differ? What criteria exist to suggest one is a good candidate for this procedure? But I was prepared for your need to modify everything related to therapy and motor function, it very much sounds like a significant re-boot following this procedure. I am saddened to hear about your struggle to return to a more normal life. Please stay strong, keep focused on trying to improve, and good luck! Frank
LikeLike
Frank,
I would highly appreciate it if you could tell me what seems to be the problem with this research. I tried to offer some money for running the duplicate experiments and there were no takers.
Recently I read a research paper by Dr. Robert Dourmashkin et al Virus-like particles and enterovirus antigen found in the brainstem neurons of Parkinson’s disease – F1000Research https://f1000research.com/articles/7-302/v2. In this article the authors describe their findings of investigating post-mortem specimens taken from 14 donors who had late onset Parkinson Disease and also from the control group of 7 who didn’t have Parkinson using transmission electron microscopy (TEM) and immunohistochemistry (IHC) . According to the authors they found evidence of virus infection (mature virus, virus factories, cells “re-cycled” by the virus and cells going through autophagy) in neurons in substantia nigra of all 14 donors. 6 specimens in the control group were virus free and only one control specimen had VLPs. Furthermore, using IHC they demonstrated that the infecting virus is likely belongs to enteroviruses.
What is your opinion of this research, Professor? If proven correct this finding would explain many features of PD, the lack of disease modifying treatments (DMT) based on current animal models, and open way for possible prevention of the disease similar to what is done for example for polio another illness caused by the enterovirus attacking neurons. I am also curious if anybody was doing broad virus related PCR screening of PD patients CSF? Assuming that Dr. Dourmashkin’s research is correct how difficult would it be to isolate the punitive virus and sequence it? Would it possible to apply methods described in your article
I find it frustrating that billions of dollars are spent on the development of treatments using animal models that have not produced a single DMT in humans yet seemed to be quite effective in treating affected animals . I think the only reasonable (and useful) conclusion that can be reached from this work is that the animal models used do not reflect PD etiology.
I would highly appreciate it if you could find a few minutes to give me your critical view of Dr. Dourmashkin’s work.
Thank you,
Felix Nedorezov
LikeLike