


“Tentative efforts lead to tentative outcome.” Epictetus
“Patients should have rest, food, fresh air, and exercise – the quadrangle of health.” William Osler
Background: The function of our spine, all the bones and muscles, and associated tissues connected to this region are crucial for everyday life. A prevalent injury or pain that many people typically have is usually to some part of the back.
Part 1 of three blog posts in the series entitled “Parkinson’s and Axial Rotation” was based on the cervical spine (click here), and Part 2 described the thoracic spine (click here). The 3rd post will focus on the lumbar spine region.* These three blog posts aim to present some exercises to help stretch specific back areas. A few other things to consider besides the actual task of exercising, one should also exercise the core region if the back is being targeted. Furthermore, one must consider your response to recovery from injury, the quality/quantity of sleep, and the quality of your overall diet plan, especially for Parkinson’s. Let’s begin with a review of the structure and function of the spine.
*Please read the medical disclaimer at the end. And as always, a reminder, I am neither a physician nor a physical therapist. Therefore, no matter how hard I try, they are trained experts. Contact them for further details about these and other exercises.
“Exercise of the muscles keeps the body in health, and exercise of the brain brings peace of mind.” John Lubbock
Regions of the Spine: We typically identify four areas of the spine, including cervical, thoracic, lumbar, and sacral. Each part of the spine has vital physiological functions that protect the body in response to physical stress and obstacles we face daily. See the figure below.
- The cervical region of the spine is the neck region. There are seven vertebrae, which are identified as C1 through C7 from top to bottom. Cervical vertebrae support the skull, protect the brain stem and the spinal cord, and support the head movement.
- The spine’s thoracic region begins where the cervical ends, and there are twelve thoracic vertebrae numbered from top to bottom as T1 through T12. Ribs attach to the thoracic vertebrae increasing their strength and offers protection for many essential organs. Thus, the thoracic range of motion is limited due to these structural features.
- The lumbar spine region begins after T12, with five vertebrae identified as L1 through L5. The lumbar region is designed and poised to bear much of the body’s weight. The lumbar vertebrae are more flexible than the thoracic spine region but less flexible than the cervical region.
- The sacral region of the spine is located behind the pelvis, numbered S1 through S5. The sacrum is a triangular-shaped region from the fusion of the sacral vertebrae. The coccyx (tailbone) is below the sacrum and is formed from the fusion of five additional bones. Think of the sacrum as a connector between the spinal cord and the pelvis. The sacrum and coccyx allow us to sit upright.

“We don’t stop playing because we grow old; we grow old because we stop playing.” George Bernard Shaw
Lumbar Spine and Back Injuries: It has been estimated that ~80% of the people living in Western countries experience lower back pain during their lifetime. Many adults, with or without Parkinson’s, are involved in some sports activity that requires rotational movement. These sports include golf, tennis, baseball/softball, pickleball, hockey, lacrosse, and cricket. These sports are called “rotational sports.” In reading through this list, they may seem quite different from one another, but their action requires lumbar spine motion. Injuries to the lumbar spine region usually involve spinal musculature, intervertebral discs, intervertebral ligaments, and vertebrae.
If you have injured the lumbar region of your spine, please consult a medical physician, get some physical therapy, and go through their prescribed rehabilitation program. My advice here does not override your physician expert, physical therapists, and their work with you because they presumably know you and your body well. However, if all else has failed, maybe try some of these exercises and move on with your rehabilitation.
“Once you learn to quit, it becomes a habit.” Vince Lombardi
Postural Instability in Parkinson’s: Posture, balance, and twisting motions of the spine (axial mobility) is the foundation upon what happens from an upright stance, walking, and many of the daily actions we complete without consciously thinking. Postural instability refers to an impairment in maintaining posture and balance, compromising the ability to quickly and efficiently maintain and change positions. Postural instability is one of the Cardinal Signs of Parkinson’s, together with bradykinesia, rigidity, and tremor, and presents in many patients at diagnosis and worsens with the progression of the disease. Since this has been repeated in Parts 1 and 2 regarding the cervical and thoracic spine regions, our continued mobility with Parkinson’s is crucial to your quality of life. Stretching and exercising is vital to your future life in the presence of this life-quenching disorder. As the Nike trademark reminds us, “Just Do It!”
“Attitude determines how well you do it.” Lou Holtz
Overview of the Stretches and Exercises of the Lumbar Spine: This blog post highlights stretching and strengthening exercises for a specific set of muscles in the lower back, the lumbar spine region. These muscles are notorious for involving the lumbar region function and the region nearest it, the hips. As mentioned in the introduction, alteration of the axial skeletal area (in this case, the lumbar spine region) will ultimately alter our ability to move, in this case, the pelvic complex.
Please note that other muscles involved in the lumbar spine region could be highlighted here, as numerous stretches and strengthening exercises; however, I have chosen these muscles because of (i) reading several reviews about rehabilitating the lumbar spine and (ii) personal experience with their dysfunction. Doing a simple Google-based search for individual muscles and stretches/exercises will reveal many additional examples.
In my early childhood-teenage years, I played baseball and softball later in life. Additionally, I was a competitive tennis player for many years (even became a professional to become an instructor for several years), and I am now returning to the game in retired life. Finally, throughout most of my life, I have played the game of golf. All four of these sports are rotational sports.
At the end of this post are several review articles related to chronic lower back pain.
“Do not let what you cannot do interfere with what you can do.” John Wooden
How to Use This Guide on the Lumbar Spine: First, if you have no lower back pain, congratulations. Performing some of the straightforward stretches of these four muscles may help maintain your back in excellent health. As always, if ANY stretch or exercise causes pain, stop. Try it again; slower, less intense motion. If the pain subsides, continue the activity. However, if the pain persists, stop.
Second, maybe your back has become sore because you have been sitting too long working on your computer. Many of these stretches and exercises can help relieve such lower back pain. My physical therapists always remind me to every 20 min of sitting, get up and do 1-2 min of stretching. It will make a difference.
Third, maybe you are a “weekend warrior” and enjoy one or more of the above-mentioned rotational sports. Perhaps the lower back pain you feel after exercising is due to a lower back injury (spine, etc. ). The goal is to strengthen the core region (not included here) and these muscle groups to help stabilize the area. This is not healing the lumbar spine region; that’s the job of the orthopedic physician, a specialist in the spine. These stretches and exercises would augment and help support the rehabilitation. Remember, seek expert help first.
The flow or work starts with the multifidus muscle, then the quadratus lumborum muscle, followed by the piriformis and psoas muscles. Remember, I write these blogs as a self-help-me-forum with the hope they help others with Parkinson’s. Specifically, I will use several of these exercises during the week because I have a documented history of lower back (lumbar region) pain.
“In golf, as in life, you get out of it what you put into it.” Sam Snead
Lumbar Multifidus Muscle:
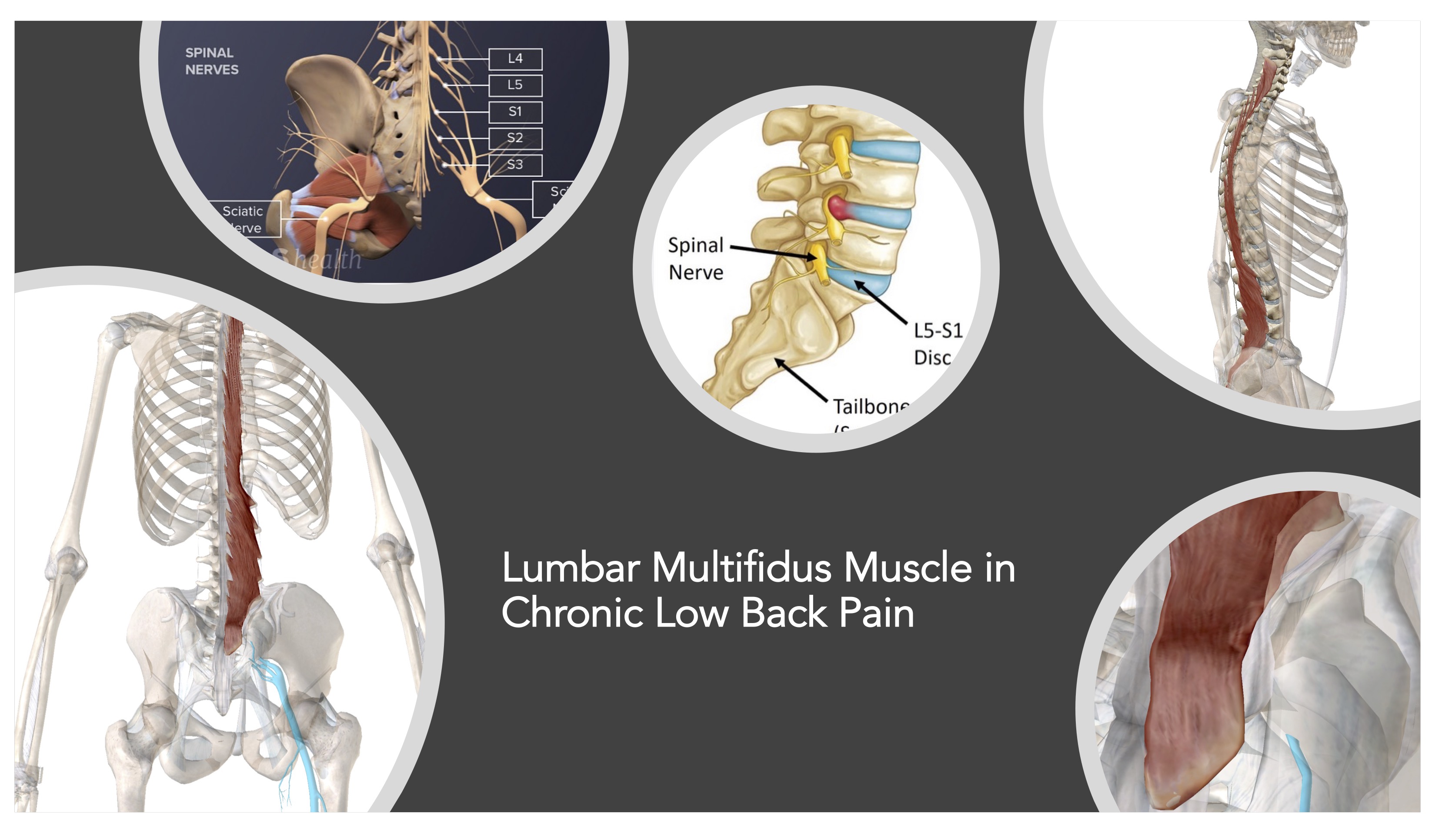
•Anatomy– Acording to Physio-pedia and Wikipedia, the multifidus muscle is a series of small, triangular muscular and tendinous bundles located on either side of the spinal column, where they fill the groove between the transverse and spinous processes of the vertebrae. The multifidus muscle spans the whole length of the vertebral column but is most developed in the lumbar region.
•Physiological Function– The multifidus muscle in the lumbar region is vital as a stabilizer. The arrangement of deep and superficial muscle fibers makes the multifidus muscle biomechanically ideal for stabilizing the lumbar area. Upon lumbar spine injury, the multifidus muscle in this region will atrophy, leading the spine to be more vulnerable to re-injury.
•Exercises– Do the “Birddog” exercise, and hold each stretch 5 seconds as demonstrated on this video (click here to view the video). Including the abdominal muscles with the multifidus muscle, here is a video with 2 exercises that will help stretch these critical muscles (click here to view video).
“Living a healthy lifestyle will only deprive you of poor health, lethargy, and fat.” Jill Johnson
Quadratus Lumborum Muscle:

•Anatomy– Acording to Physio-pedia and Wikipedia, the quadratus lumborum is the deepest back muscle and originates from the iliac crest and inserts on the transverse process of lumbar one through five and the lower part of the twelfth rib. The quadratus lumborum muscle is flattened and has a quadrangular shape. It is the deepest abdominal muscle, commonly called the back muscle.
Look at it this way, the top of the quadratus lumborum is attached to the last rib. Next, the bottom part of the quadratus lumborum is attached to the pelvic area. And the third aspect of this muscle is attached to the lumbar spine. Thus, many different movements of the body involve the quadratus lumborum muscle, and following injury, it would be important to rehabilitate it due to its dynamic sites of interactions.
•Physiology– Physio-pedia lists several primary functions for the quadratus lumborum muscle, including lateral flexion of the vertebral column, with ipsilateral contraction. Extension of the lumbar vertebral column, with bilateral contraction. Fixes the 12th rib during forced expiration. The quadratus lumborum assists the diaphragm in inhalation. Also, it elevates the ilium (bone) with ipsilateral contractions (“hip hiking”).
•Exercises– Do the “Open Book” exercise (click here for an overview of this exercise); place a lacrosse ball on the ground and place the sore spot in your lower back on the ball (but not your spine); some of the exercises here may be beneficial (click here to view video); and finally, do the Thomas Stretch (click here for a demonstration).
“I have two doctors, my left leg and my right.” G. M. Trevelyan
Piriformis Muscle:
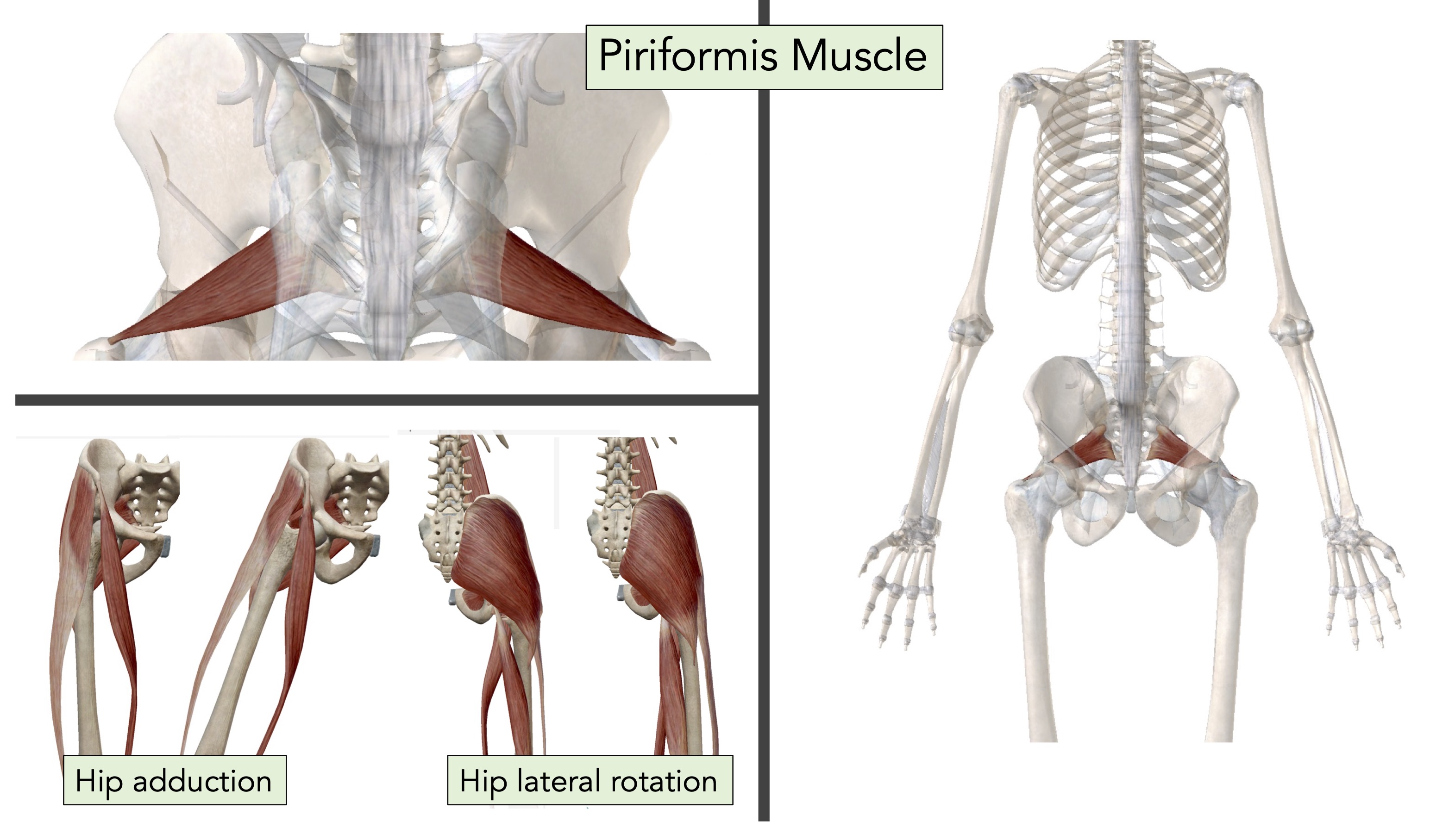
•Anatomy– Acording to Physio-pedia and Wikipedia, the piriformis muscle is a flat muscle and the most superficial muscle of the deep gluteal muscles. It is part of the lateral rotators of the hip (obturator internus, superior and inferior gemelli, quadratus femoris, obturator externus, and gluteus maximus). It leaves the pelvis through the greater sciatic notch, until its fixation reaches the superior margin of the greater trochanter. It has a pyramidal shape that lies almost parallel with the posterior margin of the gluteus medius.
•Physiology– The piriformis muscle is an external (or lateral) rotator of the hip. The piriformis muscle rotates the femur during the hip extension and abducts the femur during flexion of the hip. The piriformis has several functions including, Lateral rotation of the hip when it is extended (that is when in standing); aduction of the hip when it is flexed.; aids slightly in tilting pelvis laterally; and aids in tilting pelvis posteriorly by pulling the sacrum down towards the thigh. The piriformis muscle can be used to locate the sciatic nerve. If the lateral rotators of the hip are tight they may exert pressure on the sciatic nerve, producing pain radiating into the lower extremity, which is called Piriformis Syndrome.
•Exercises– This simple stretch targets the piriformis and can begin to alleviate any pain with this muscle (watch the stretching exercise that starts at 6:30 min, click here for video; you may find some of the other stretches shown here beneficial as well). Here are some additional exercises to stretch the piriformis, and it is closely liked to sciatica (click here to view video).
“I am sick and tired of being sick and tired.” Fannie Lou Hamer
Psoas Muscle (Major and Minor):

•Anatomy– The psoas muscle attaches to the vertebrae on the lumbar spine, and then crosses the outer edge of each pubis (near your pelvis). It next joins with the iliacus muscle at the inguinal ligament (in your groin region), and finally attaches at the femur. The iliacus and psoas muscles are together known as the iliopsoas.
•Physiology– We have three muscles that connect our spine to our legs, including the gluteus maximus, piriformis, and psoas muscles. You can stand and walk upright in part because the curve of your lower spine bears and transfers the weight above it. The psoas muscle helps create this curve, pulling your lumbar vertebrae forward and down. The psoas muscle also plays another essential role in helping you walk. When walking, your brain triggers your psoas muscle to move your back leg forward—initiating the alternation between the front and back leg. So each successful step you take is thanks in part to your psoas muscle.
•Exercises– The first video highlighted here is quite informative about combining anatomy, physiology, and useful stretches for the psoas muscle (the stretches begin at 4:04 min, click here to view video). Another video with 7 stretches for the psoas muscle (click here to view video).
“Health is worth more than learning.” Thomas Jefferson
Medical Disclaimer Statement on Performing these Exercises
MEDICAL DISCLAIMER: Always consult your physician before beginning any exercise program. This general information is not intended to diagnose any medical condition or to replace your healthcare professional. Consult with your healthcare professional to design an appropriate exercise prescription. If you experience any pain or difficulty with these exercises, stop and consult your healthcare provider.
WHEN TO CONTACT YOUR PHYSICIAN: If you experience any symptoms of weakness, unsteadiness, light-headedness or dizziness, chest pain or pressure, nausea, or shortness of breath. Mild soreness after exercise may be experienced after beginning a new exercise. Contact your physician if the soreness does not improve after 2-3 days.
Useful References to Chronic Low Back Pain and the Specific Muscles Described Above:
Freeman, Michael D., Mark A. Woodham, and Andrew W. Woodham. “The role of the lumbar multifidus in chronic low back pain: a review.” Pm&r 2, no. 2 (2010): 142-146.
Li, Wei, Yinan Gong, Jingyi Liu, Yongming Guo, Huiling Tang, Siru Qin, Yadan Zhao, Songtao Wang, Zhifang Xu, and Bo Chen. “Peripheral and central pathological mechanisms of chronic low back pain: a narrative review.” Journal of Pain Research (2021): 1483-1494.
Hansen, Lone, Mark De Zee, John Rasmussen, Thomas B. Andersen, Christian Wong, and Erik B. Simonsen. “Anatomy and biomechanics of the back muscles in the lumbar spine with reference to biomechanical modeling.” Spine 31, no. 17 (2006): 1888-1899.
Neumann, D. A. “Axial skeleton: muscle and joint interactions.” Kinesiology of the Musculoskeletal System. 2nd ed. St Louis: Mosby (2010): 379-422.
Urits, Ivan, Aaron Burshtein, Medha Sharma, Lauren Testa, Peter A. Gold, Vwaire Orhurhu, Omar Viswanath et al. “Low back pain, a comprehensive review: pathophysiology, diagnosis, and treatment.” Current pain and headache reports 23 (2019): 1-10.
Schenkman, Margaret, Kathy M. Shipp, Julie Chandler, Stephanie A. Studenski, and Maggie Kuchibhatla. “Relationships between mobility of axial structures and physical performance.” Physical therapy 76, no. 3 (1996): 276-285.
“I train like I’m training for the Olympics or for a Mr. America contest, the way I’ve always trained my whole life. You see, life is a battlefield. Life is survival of the fittest… How many healthy people do you know? How many happy people do you know? Think about it. People work at dying, they don’t work at living. My workout is my obligation to life. It’s my tranquilizer. It’s part of the way I tell the truth–and telling the truth is what’s kept me going all these years.” Jack LaLanne
Cover Photo Image by Kerryanna Kershner from Pixabay
