


“I never think of the future – it comes soon enough.” Albert Einstein
“We are made wise not by the recollection of our past, but by the responsibility for our future.” George Bernard Shaw
Describing Some of the Science Behind Using Supplements to Treat Parkinson’s: There are many ways to start and defend this section. One way would be to say there are hundreds of choices of supplements to “potentially” treat Parkinson’s. My concern about some of these substances is not that they don’t work but whether they are considered safe to consume and whether they have been tested for heavy metals and other potential toxins. Ayurvedic medicine for many centuries has targeted the brain. Personally and philosophically, it is hard to beat medicinal herbs and supplements used for centuries. Slowly, some of these compounds, e.g., Ashwagandha and tumeric/curcumin (and many others), are becoming mainstream over-the-counter products.
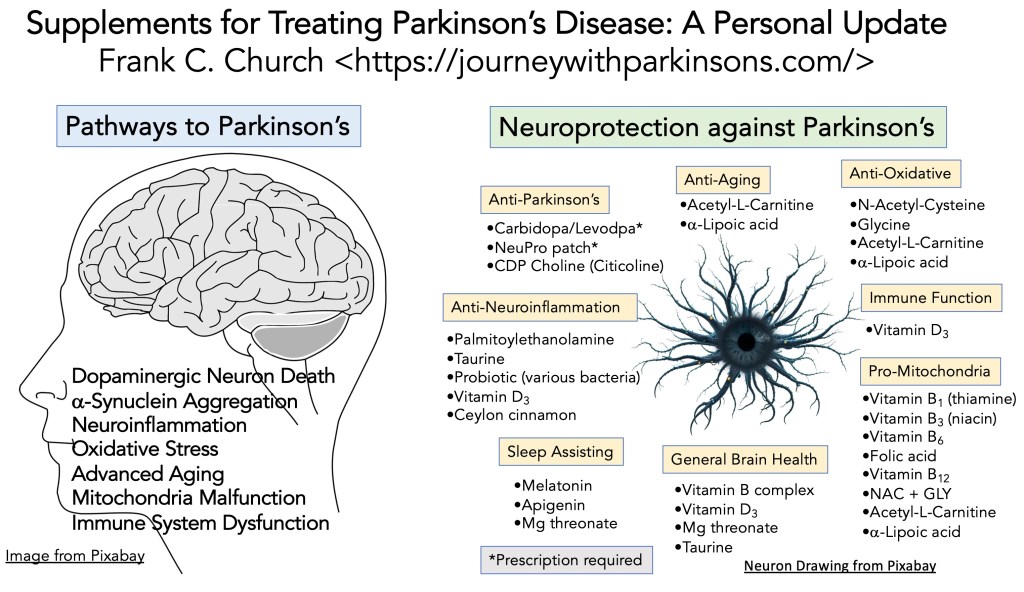
I like to use schematics and graphs to help me understand things. We are learning much about the pathways that support the development of Parkinson’s. There are a bunch of pathways; see the schematic below. Therefore, one valuable approach is to target a pathway, e.g., neuroinflammation, and take supplements that could contribute to down-regulating this process. Here is where it gets tricky for me. There are many different paths to starting Parkinson’s. Does that mean they all contribute some to the genesis of Parkinson’s? If so, can we assign a percentage for each in their role (implying that some of these pathways are more involved or important than others)? Or does this mean that a single path predominates in an individual who develops Parkinson’s and the others play very minor roles? But this is all speculation; the schematic shows the many different paths taken in the genesis and progression of Parkinson’s. Overall, we should strive to improve the general health of the brain and taking supplements to hopefully re-focus the disease transition that is occurring from Parkinson’s.
“What you do today can change all the tomorrow’s of your life.” Zig Ziglar
A Personal Choice for Using Supplements to Treat Parkinson’s: Some of you say to ignore supplements; all you need to do is eat right, exercise a lot, and sleep well (besides taking prescribed therapies). And I do value this opinion. I guess my reason for taking supplements is if they help in slowing down the progression of my disorder by, let’s say, 5-10%, then it is worth it [5-10% of 83 years (just a guess to how many years I may live) is (0.05) * 83 = ~4 years and (0.10) * 83= ~8 years. Adding those 4-8 years to your 83 years gives you a potential lifespan of 87 to 91 years]. Taking a chance by helping to improve my health is the main reason I am taking supplements.
My approach is to broadly target the use of supplements that can help and not hinder other pharmaceutical prescriptions that are known to be effective in treating Parkinson’s. So far, we have no cure for Parkinson’s. Thus, instead of waiting for this ‘miracle to happen,’ I take a focused approach to trying to manage my Parkinson’s. These compounds might help to treat the disorder. I am not afraid to add other supplements, remove some from the current stack, or go back and further refine my opinion about given compounds. Unless there is a dramatic change in motor score, one may not feel any different over time. That is a conundrum: how does one know whether a supplement works?
Consider this: if you have not increased your carbidopa/levodopa amount in several years, then might this be considered a prolongation of your life-time with Parkinson’s? Success? Are you slowing down the progression of your disorder by taking supplements? Or is that total nonsense?I do not have the answer. I am only an n = 1, but I know there are a lot of you out there doing the same thing, taking supplements with the hope that you are slowing down the beast named Parkinson’s. I admire your dedication and willingness to experiment. I wish you the best of luck in this pursuit.
“Finish each day and be done with it. You have done what you could. Some blunders and absurdities no doubt crept in; forget them as soon as you can. Tomorrow is a new day; begin it well and serenely and with too high a spirit to be encumbered with your old nonsense.” Ralph Waldo Emerson
Overview of a Selection of Supplements for Parkinson’s: What follows below can be split into two presentations. The first section presents the usual update of my treatment strategy for using supplements to treat Parkinson’s. If you have any questions, please write; I would be happy to provide feedback and support you have about any of these supplements described here. The following part is a list of some of the many supplements (given here is just a tiny percentage of what is available). This list is divided up into the categories from the schematic above [sections include Biological Action and Literature Citations, and Adverse Reactions (many of the adverse reaction responses were obtained from Google/AI-assisted searches)].
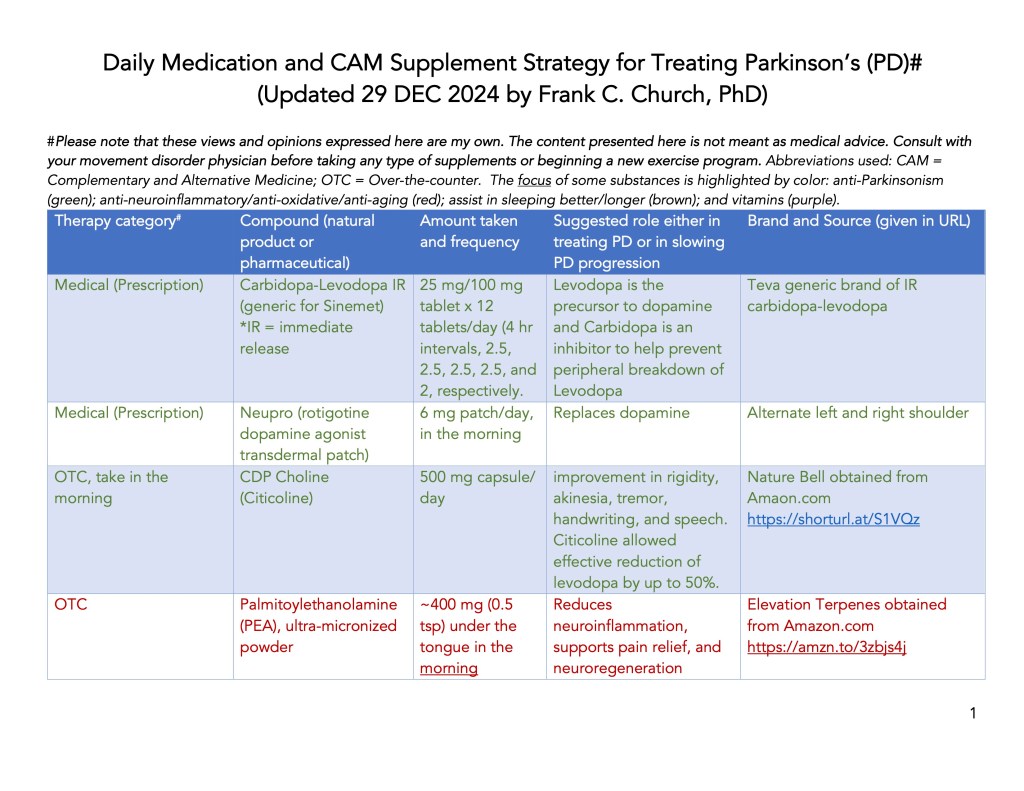
Supplement List, Daily Amount Taken, and the Source of Supplements:
Download the 4-page handout in PDF format (updated 12/29/2024) by clicking here.

Anti-Parkinson’s Prescription Drugs and Supplements:
| Prescription* or Supplement | Biological Action | Adverse Reactions | Reference(s) [are at the end of the blog] |
| *Carbidopa/Levodopa | Levodopa is the precursor to dopamine, and Carbidopa is an inhibitor to help prevent the peripheral breakdown of Levodopa | It may cause dizziness, lightheadedness, and fainting when you get up too quickly from a lying position. It may cause involuntary movement problems, including shakiness, stiffness, or jerkiness. | Ahlskog, J.E. (2015) |
| *NeuPro (rotigotine dopamine agonist transdermal patch) | It acts as a dopamine receptor agonists, primarily binds to D1, D2, and D3. | The most serious adverse effects include compulsive behavior, gambling and hypersexuality. | Church, F.C. (2021) |
| CDP Choline (Citicoline) | It may impact dopamine synthesis, increase dopamine receptors, and reduce carbidopa /levodopa needed over time. | .Nausea, Constipation, Headache or Insomnia, Hypotension, Blurred vision, or Restlessness. Interestingly, the FDA held up the sales of the supplement (a few years ago) see letter here. | Agnoli et al. (1982) Cubells et al. (1988) |
Anti-Neuroinflammatory Supplements:
| Supplement | Biological Action | Adverse Reactions | Reference(s) [are at the end of the blog] |
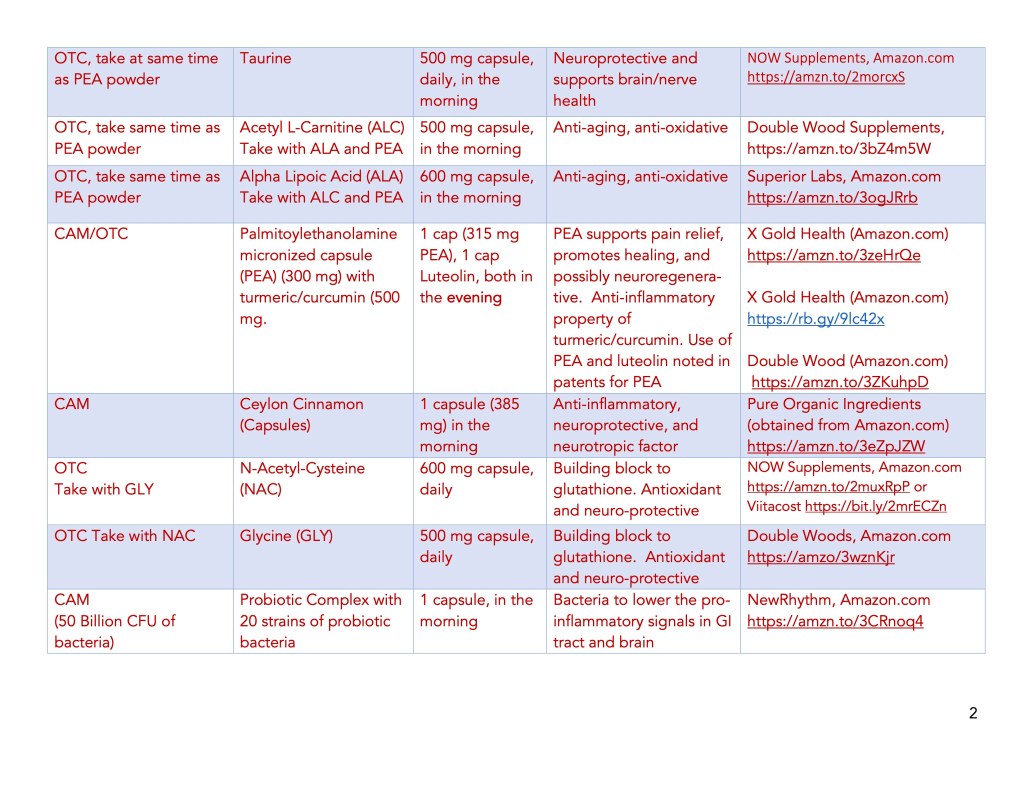
| Taurine | Reduced in human PD vs. age-matched controls. It lowers microglial cell activation. Protects dopaminergic neurons and reduces neuropathy (in diabetes). | Long-term use has not been studied. It is safe when used as a medicine for up to 3 months. It may lower blood pressure by interacting with anti-hypertensive drugs. | Zhang et al. (2016) Che et al.(2018) WebMD citation Jangra et al. (2024) |
| Palmitoylethanol-amine (PEA) | Reduces microglial and astrocyte activation and oxidative stress. PEA has been found to reduce interferon-γ, tumor necrosis factor-α, and interleukin-17. It was also clinically shown to improve motor symptoms in advanced PD. | PEA may cause a heavy feeling in the stomach, and, when taken sublingually, may cause minor gastrointestinal disturbance. Recently, PEA was shown to be protective of the kidneys. | Brotini et al. (2017) Orefice et al. (2016) Landolfo et al. (2022) Hesselink et al. (2012 Dubey et al. (2024) |
Palmitoylethanol-amine (PEA) + Luteolin, and PEA + Turmeric Curcumin | A clinica study has found that PEA and luteolin have complementary pharmacodynamic properties. They both are anti-inflammatory and can reduce oxidative stress. | There have been no long-term studies with PEA; however, Brotini et al. (2017) found that patients were on PEA for at least 12 months. | Cordaro et al. (2020) |
| Vitamin D3 | vitamin D3 has anti-inflammatory effects: it reduces pro-inflammatory cytokines, inhibits NFκB pathway, modulates immune cell activity, and reduces leukocyte migration. | Too much vitamin D can cause high calcium levels, which can lead to nausea/vomiting, constipation, increased thirst, increased urination, and kidney disease. | Krajewska et al. (2022) Mousa et al. (2017) Leal et al. (2020) |
| Ceylon cinnamon | The bioactive substance, cinnamaldehyde, is converted to benzoate in the liver, which reduces both inflammation (NF-kB) and nitric oxide and also increases BDNF levels. Ceylon cinnamon provides dopaminergic neuronal protection and improved motor functions | If taking large quantities, ensure it is Ceylon cinnamon and not Cassia cinnamon (which contains the anticoagulant coumarin). Cinnamon can interact with antibiotics, diabetes drugs, and heart medicines. | Khasnavis et al. (2014) Paphan and Pahan (2015) Angelopoulou et al (2021) |
| Probiotic | Probiotics are mixtures of bacterial strains thought to be beneficial for the human gut microflora. Probiotics can modulate. the immune system lowers nF-kB activation and reduces a key marker of inflammation, C–reactive protein (CRP). | These probiotics have anti-inflammatory properties: Lactobacillus reuteri; Lactobacillus casei; Lactobacillus bulgaricus; Bifidobacterium; Kefir; Kombucha; Tempeh; Kimchi | Plaza-Díaz et a. (2017) Seo et al. (2021) Cristofori et al. (2021) |
Anti-Aging Supplements:
| Supplement | Biological Action | Adverse Reactions | Reference(s) |
| Acetyl- l-Carnitine (ALC) | It has neuroprotective properties, and it may boost cognitive function. ALC partially restored mitochondria function in aged rodents. | ALC can cause diarrhea, nausea, stomach pain, and vomiting, insomnia, increased blood pressure, lower blood sugars (so be cautious if you have diabetes). | Rosca et al. (2009) |
| a-Lipoic acid (ALA) | Alpha-lipoic acid is a cofactor for some mitochondrial enzymes and functions as an antioxidant in the brain. Aged-rodents were more responsive to ALA than younger animals. | ALA can lower blood sugar levels, so people with diabetes should take it only under the supervision of their healthcare provider. | `Shanaida et al. (2024) |
Immune Function Supplement:
| Supplement | Biological Action | Adverse Reactions | Reference(s) |
| Vitamin D3 | Vitamin D3 can modulate immune cell function, promote the innate immune system while inhibiting the adaptive response, and inhibit an autoimmune response. | Too much vitamin D3 can lead to nausea and vomiting, poor appetite, and weight loss. constipation. weakness, kidney stones, and kidney damage. | Martens et al. (2020 Daryabor et al.(2023) |
Anti-Oxidative Supplements:
| Supplement | Biological Action | Adverse Reactions | Reference(s) |
| N-Acetyl Cysteine (NAC) | NAC and GLY are precursors to glutathione (GSH), the master anti-oxidative compound. Long-term use of NAC in a PD mouse model reduced neuronal loss, oxidative stress and improved motor abnormalities. | NAC has a free sulfhydryl group, and the ‘sulfur-like odor’ can make some people queasy. Otherwise, no evidence exists that NAC harms the body; however, further studies are needed to prove its safety. | Coles et al. (2018) Caridade-Silva et al. (2023) Hagen et al. (1998) |
| Glycine (GLY) | The key anti-oxidant in cells is GSH, which quickly oxidizes outside the cell to GSSG. GLY and NAC work to produce GSH, with GLU to complete the synthesis of GSH. | Side effects of GLY include Stomach discomfort. Soft stools. Nausea. | Kumar et al. (2022) McCarty et al. (2018) Kumar et al. (2023) |
| Acetyl-L-Carnitine (ALC) | It is an antioxidant that protects cells from oxidative stress by improving mitochondrial function and reducing free radical production. | ALC can cause diarrhea, nausea, stomach pain, and vomiting, insomnia, increased blood pressure, lower blood sugars (so be cautious if you have diabetes. | Wang et al. (2020) Grossini et al. (2023) |
| a-Lipoic acid (ALA) | ALA is a potent anti-oxidant due to its ability to scavenge free radicals, regenerate anti-oxidants, , | ALA can lower blood sugar levels, so people with diabetes should take it only under the supervision of their healthcare provider. | Packer et al., (1995) Capece et al. (2022) |
Sleep Assisting:
| Supplement | Biological Action | Adverse Reactions | Reference(s) |
| Melatonin | The pineal gland makes melatonin. As we age, we produce less melatonin, which helps promote sleep and regulates the circadian cycle. | Side effects include vivid dreams or nightmares, depression, irritability, constipation, or decreased appetite. | Iftikhar et al. (2023) Ma et al. (2022) |
| Apigenin | The data on humans are limited, but in rodents, it increased the levels of sleep-promoting proteins (BDNF, CREB, and serotonin), and decreased the levels of stress-related proteins . | High doses of apigenin may cause stomach disturbances. | Kramer et al. (2024) Salehi et al. (2019) |
| Mg threonate (Magtein) | Magtein passes through the blood-brain barrier, promoting a higher sleep quality. | Adverse effects range from vomiting and diarrhea to cardiac arrhythmia and shortness of breath. | Ray (2024) Zhang (2022) |
General Brain Health:
| Supplement | Biological Action | Adverse Reactions | Reference(s) |
| Vitamin B Complex | B1 (thiamine), B6 (pyridoxyl phosphate), and B12 (cobalamin), are essential for maintaining a healthy nervous system. | Vomiting, diarrhea, and flushing of skin. | Calderón-Ospina t al. (2020) |
| Vitamin D3 | Vitamin D3 is neuroprotective, helps the brain to successfully age, and low levels are linked to Parkinson’s. | Ranges from nausea and constipation to kidney disease and bone pain. | Anjum et al. (2018) |
| Magnesium threonate (Magtein) | Magnesium (Mg) helps your muscles relax and reduces motor defects in Parkinson’s. | Adverse effects range from vomiting and diarrhea to cardiac arrhythmia and shortness of breath. | Ray (2024) |
| Taurine | Taurine protects neurons from inflammation and apoptosis. It may also help maintain cognitive ability. | The safe range of taurine is not well understood, but excesses lead to vomiting, nausea, and liver pain. | Jangra et al. (2024) |
Pro-Mitochondria:
| Supplement | Biological Action | Adverse Reactions | Reference(s) |
| Vitamin B1 | Vitamin B1, also known as thiamine, is a water-soluble vitamin. Thiamine is a cofactor for several mitochondrial enzymes that produce energy, leading to adenosine triphosphate (ATP) production. ATP is critical for mitochondrial energetics. | Thiamine is considered safe in excess, although it may cause an upset stomach. There are many following a high-dose protocol where up to 4 grams per day of thiamine is taken for treating Parkinson’s. | Mrowicka et al. (2023) |
| Vitamin B3 | Vitamin B3 is also known as niacin, a water-soluble vitamin. Niacin is a cofactor for NAD synthesis, which is important for oxidative phosphorylation (i.e., energy). | High doses of niacin cause flushing (a tingling sensation in the face, neck, and chest). Those taking a statin should carefully consider the dose of niacin being taken due to a detrimental effect on the statin. | Williams et al. (2017) |
| Vitamin B6 | Vitamin B6, also known as pyridoxal phosphate (PLP), is a water-soluble vitamin. PLP is a cofactor for several mitochondrial enzymes that are involved in energy production and DNA repair. | High doses of B6 may inactivate carbidopa, which could compromise the transport of levodopa through peripheral circulation. High doses can also cause peripheral neuropathy (tingling, burning, or numbness in the hands or feet). | Kannan et al. (2004) |
| Folic acid (vitamin B9) | Folate is a water-soluble B vitamin. It is critical for protein synthesis and is involved in the electron transport chain system, which is crucial for energy production. | Higher doses of folate (>1 mg/day) may cause stomach upset, nausea, diarrhea, irritability, confusion, and seizures. | Zheng and Cantley (2019) |
| Vitamin B12 (Colamin) | Vitamin B12, also known as cobalamin, is a water-soluble B vitamin. B12 is vital for mitochondrial function; thus, B12 is essential for aiding mitochondrial health, energetics, and function. | Usually, high levels of vitamin B12 do not pose a health effect. Large amounts of injected vitamin B12 can cause low potassium, heart failure, or even blood clots. | Mukherjee et al. (2023) |
| NAC and GLY | see above information | ||
| ALC | see above information | ||
| ALA | see above information |
“Remember the past, plan for the future, but live for today, because yesterday is gone and tomorrow may never come.” Luke the Evangelist
References Cited Above:
Ahlskog, J.E. The New Parkinson’s Disease Treatment Book: Partnering with Your Doctor to Get the Most from Your Medications; Oxford University Press: Oxford, UK, 2015.
Church, F.C. Treatment Options for Motor and Non-Motor Symptoms of Parkinson’s Disease. Biomolecules 2021, 11, 612
Agnoli A, Ruggieri S, Denaro A, Bruno G. New strategies in the management of Parkinson’s disease: a biological approach using a phospholipid precursor (CDP-choline). Neuropsychobiology. 1982;8(6):289-96. doi: 10.1159/000117914. PMID: 7162583.
Cubells JM, Hernando C. Clinical trial on the use of cytidine diphosphate choline in Parkinson’s disease. Clin Ther. 1988;10(6):664-71. PMID: 3064905.
Zhang L, Yuan Y, Tong Q, Jiang S, Xu Q, Ding J, Zhang L, Zhang R, Zhang K. Reduced plasma taurine level in Parkinson’s disease: association with motor severity and levodopa treatment. Int J Neurosci. 2016;126(7):630-6. doi: 10.3109/00207454.2015.1051046. Epub 2015 Aug 18. PMID: 26004911.
Che, Y., Hou, L., Sun, F. et al. Taurine protects dopaminergic neurons in a mouse Parkinson’s disease model through inhibition of microglial M1 polarization. Cell Death Dis 9, 435 (2018). https://doi.org/10.1038/s41419-018-0468-2
Jangra A, Gola P, Singh J, Gond P, Ghosh S, Rachamalla M, Dey A, Iqbal D, Kamal M, Sachdeva P, Jha SK, Ojha S, Kumar D, Jha NK, Chopra H, Tan SC. Emergence of taurine as a therapeutic agent for neurological disorders. Neural Regen Res. 2024 Jan;19(1):62-68. doi: 10.4103/1673-5374.374139. PMID: 37488845; PMCID: PMC10479846.
https://www.webmd.com/vitamins/ai/ingredientmono-1024/taurine
Brotini S, Schievano C, Guidi L. Ultra-micronized Palmitoylethanolamide: An Efficacious Adjuvant Therapy for Parkinson’s Disease. CNS Neurol Disord Drug Targets. 2017;16(6):705-713. doi: 10.2174/1871527316666170321124949. PMID: 28325153.
Orefice NS, Alhouayek M, Carotenuto A, Montella S, Barbato F, Comelli A, Calignano A, Muccioli GG, Orefice G. Oral Palmitoylethanolamide Treatment Is Associated with Reduced Cutaneous Adverse Effects of Interferon-β1a and Circulating Proinflammatory Cytokines in Relapsing-Remitting Multiple Sclerosis. Neurotherapeutics. 2016 Apr;13(2):428-38. doi: 10.1007/s13311-016-0420-z. PMID: 26857391; PMCID: PMC4824021.
Landolfo E, Cutuli D, Petrosini L, Caltagirone C. Effects of Palmitoylethanolamide on Neurodegenerative Diseases: A Review from Rodents to Humans. Biomolecules. 2022 May 5;12(5):667. doi: 10.3390/biom12050667. PMID: 35625595; PMCID: PMC9138306.
Hesselink JM, Hekker TA. Therapeutic utility of palmitoylethanolamide in the treatment of neuropathic pain associated with various pathological conditions: a case series. J Pain Res. 2012;5:437-42. doi: 10.2147/JPR.S32143. Epub 2012 Oct 26. PMID: 23166447; PMCID: PMC3500919.
Dubey V, Kansagra J, Kamani B, Sureja V. Protective and Therapeutic Efficacy of Palmitoylethanolamide in Diabetes Induced Renal Damage: A Narrative Review of Scientific Evidences. Arch Nephrol Ren Stud. 2024;4(1):8-13.
Cordaro M, Cuzzocrea S, Crupi R. An Update of Palmitoylethanolamide and Luteolin Effects in Preclinical and Clinical Studies of Neuroinflammatory Events. Antioxidants (Basel). 2020 Mar 5;9(3):216. doi: 10.3390/antiox9030216. PMID: 32150935; PMCID: PMC7139331.
Khasnavis S, Pahan K. Cinnamon treatment upregulates neuroprotective proteins Parkin and DJ-1 and protects dopaminergic neurons in a mouse model of Parkinson’s disease. J Neuroimmune Pharmacol. 2014 Sep;9(4):569-81. doi: 10.1007/s11481-014-9552-2. Epub 2014 Jun 20. PMID: 24946862; PMCID: PMC4167597.
Pahan P, Pahan K. Can cinnamon bring aroma in Parkinson’s disease treatment? Neural Regen Res. 2015 Jan;10(1):30-2. doi: 10.4103/1673-5374.150647. PMID: 25788911; PMCID: PMC4357107.
Angelopoulou, E.; Paudel, Y.N.; Piperi, C.; Mishra, A. Neuroprotective potential of cinnamon and its metabolites in Parkinson’s disease: Mechanistic insights, limitations, and novel therapeutic opportunities. Journal of Biochemical and Molecular Toxicology 2021, 35, e22720, doi:https://doi.org/10.1002/jbt.22720.
Krajewska, M.; Witkowska-Sędek, E.; Rumińska, M.; Stelmaszczyk-Emmel, A.; Sobol, M.; Majcher, A.; Pyrżak, B. Vitamin D Effects on Selected Anti-Inflammatory and Pro-Inflammatory Markers of Obesity-Related Chronic Inflammation. Frontiers in Endocrinology 2022, 13, doi:10.3389/fendo.2022.920340.
Mousa, A., Naderpoor, N., Johnson, J. et al. Effect of vitamin D supplementation on inflammation and nuclear factor kappa-B activity in overweight/obese adults: a randomized placebo-controlled trial. Sci Rep 7, 15154 (2017). https://doi.org/10.1038/s41598-017-15264-1
Moreira Leal, L.K.; Lima, L.A.; Alexandre de Aquino, P.E.; Costa de Sousa, J.A.; Jataí Gadelha, C.V.; Felício Calou, I.B.; Pereira Lopes, M.J.; Viana Lima, F.A.; Tavares Neves, K.R.; Matos de Andrade, G.; et al. Vitamin D (VD3) antioxidative and anti-inflammatory activities: Peripheral and central effects. European Journal of Pharmacology 2020, 879, 173099, doi:https://doi.org/10.1016/j.ejphar.2020.173099.
Plaza-Díaz J, Ruiz-Ojeda FJ, Vilchez-Padial LM, Gil A. Evidence of the Anti-Inflammatory Effects of Probiotics and Synbiotics in Intestinal Chronic Diseases. Nutrients. 2017 May 28;9(6):555. doi: 10.3390/nu9060555. PMID: 28555037; PMCID: PMC5490534.
Seo, H.; Seong, H.; Kim, G.Y.; Jo, Y.M.; Cheon, S.W.; Song, Y.; Ryu, B.H.; Kang, H.; Han, N.S. Development of Anti-inflammatory Probiotic Limosilactobacillus reuteri EFEL6901 as Kimchi Starter: in vitro and In vivo Evidence. Frontiers in Microbiology 2021, 12, doi:10.3389/fmicb.2021.760476.
Cristofori F, Dargenio VN, Dargenio C, Miniello VL, Barone M, Francavilla R. Anti-Inflammatory and Immunomodulatory Effects of Probiotics in Gut Inflammation: A Door to the Body. Front Immunol. 2021 Feb 26;12:578386. doi: 10.3389/fimmu.2021.578386. PMID: 33717063; PMCID: PMC7953067.
Rosca MG, Lemieux H, Hoppel CL. Mitochondria in the elderly: Is acetylcarnitine a rejuvenator? Adv Drug Deliv Rev. 2009 Nov 30;61(14):1332-1342. doi: 10.1016/j.addr.2009.06.009. Epub 2009 Aug 29. PMID: 19720100; PMCID: PMC4120470.
Shanaida M, Lysiuk R, Mykhailenko O, Hudz N, Abdulsalam A, Gontova T, Oleshchuk O, Ivankiv Y, Shanaida V, Lytkin D, Bjørklund G. Alpha-lipoic Acid: An Antioxidant with Anti-Aging Properties for Disease Therapy. Curr Med Chem. 2024 Apr 19. doi: 10.2174/0109298673300496240416114827. Epub ahead of print. PMID: 38644711.
Hagen TM, Ingersoll RT, Wehr CM, Lykkesfeldt J, Vinarsky V, Bartholomew JC, Song MH, Ames BN. Acetyl-L-carnitine fed to old rats partially restores mitochondrial function and ambulatory activity. Proc Natl Acad Sci U S A. 1998 Aug 4;95(16):9562-6. doi: 10.1073/pnas.95.16.9562. PMID: 9689120; PMCID: PMC21378.
Coles LD, Tuite PJ, Öz G, Mishra UR, Kartha RV, Sullivan KM, Cloyd JC, Terpstra M. Repeated-Dose Oral N-Acetylcysteine in Parkinson’s Disease: Pharmacokinetics and Effect on Brain Glutathione and Oxidative Stress. J Clin Pharmacol. 2018 Feb;58(2):158-167. doi: 10.1002/jcph.1008. Epub 2017 Sep 22. PMID: 28940353; PMCID: PMC5762253.
Caridade-Silva R, Araújo B, Martins-Macedo J, Teixeira FG. N-Acetylcysteine Treatment May Compensate Motor Impairments through Dopaminergic Transmission Modulation in a Striatal 6-Hydroxydopamine Parkinson’s Disease Rat Model. Antioxidants (Basel). 2023 Jun 11;12(6):1257. doi: 10.3390/antiox12061257. PMID: 37371987; PMCID: PMC10295771.
Kumar P, Osahon OW, Sekhar RV. GlyNAC (Glycine and N-Acetylcysteine) Supplementation in Mice Increases Length of Life by Correcting Glutathione Deficiency, Oxidative Stress, Mitochondrial Dysfunction, Abnormalities in Mitophagy and Nutrient Sensing, and Genomic Damage. Nutrients. 2022 Mar 7;14(5):1114. doi: 10.3390/nu14051114. PMID: 35268089; PMCID: PMC8912885.
McCarty MF, O’Keefe JH, DiNicolantonio JJ. Dietary Glycine Is Rate-Limiting for Glutathione Synthesis and May Have Broad Potential for Health Protection. Ochsner J. 2018 Spring;18(1):81-87. PMID: 29559876; PMCID: PMC5855430.
Kumar P, Liu C, Suliburk J, Hsu JW, Muthupillai R, Jahoor F, Minard CG, Taffet GE, Sekhar RV. Supplementing Glycine and N-Acetylcysteine (GlyNAC) in Older Adults Improves Glutathione Deficiency, Oxidative Stress, Mitochondrial Dysfunction, Inflammation, Physical Function, and Aging Hallmarks: A Randomized Clinical Trial. J Gerontol A Biol Sci Med Sci. 2023 Jan 26;78(1):75-89. doi: 10.1093/gerona/glac135. PMID: 35975308; PMCID: PMC9879756.
Wang S, Xu J, Zheng J, Zhang X, Shao J, Zhao L, Hao J. Anti-Inflammatory and Antioxidant Effects of Acetyl-L-Carnitine on Atherosclerotic Rats. Med Sci Monit. 2020 Jan 16;26:e920250. doi: 10.12659/MSM.920250. PMID: 31945029; PMCID: PMC6984015.
Grossini E, De Marchi F, Venkatesan S, Mele A, Ferrante D, Mazzini L. Effects of Acetyl-L-Carnitine on Oxidative Stress in Amyotrophic Lateral Sclerosis Patients: Evaluation on Plasma Markers and Members of the Neurovascular Unit. Antioxidants (Basel). 2023 Oct 20;12(10):1887. doi: 10.3390/antiox12101887. PMID: 37891966; PMCID: PMC10604350.
Packer L, Witt EH, Tritschler HJ. alpha-Lipoic acid as a biological antioxidant. Free Radic Biol Med. 1995 Aug;19(2):227-50. doi: 10.1016/0891-5849(95)00017-r. PMID: 7649494.
Capece U, Moffa S, Improta I, Di Giuseppe G, Nista EC, Cefalo CMA, Cinti F, Pontecorvi A, Gasbarrini A, Giaccari A, Mezza T. Alpha-Lipoic Acid and Glucose Metabolism: A Comprehensive Update on Biochemical and Therapeutic Features. Nutrients. 2022 Dec 21;15(1):18. doi: 10.3390/nu15010018. PMID: 36615676; PMCID: PMC9824456.
Martens PJ, Gysemans C, Verstuyf A, Mathieu AC. Vitamin D’s Effect on Immune Function. Nutrients. 2020 Apr 28;12(5):1248. doi: 10.3390/nu12051248. PMID: 32353972; PMCID: PMC7281985.
Daryabor G, Gholijani N, Kahmini FR. A review of the critical role of vitamin D axis on the immune system. Exp Mol Pathol. 2023 Aug;132-133:104866. doi: 10.1016/j.yexmp.2023.104866. Epub 2023 Aug 17. PMID: 37572961.
Iftikhar S, Sameer HM, Zainab. Significant potential of melatonin therapy in Parkinson’s disease – a meta-analysis of randomized controlled trials. Front Neurol. 2023 Oct 10;14:1265789. doi: 10.3389/fneur.2023.1265789. PMID: 37881313; PMCID: PMC10597669.
Ma H, Yan J, Sun W, Jiang M, Zhang Y. Melatonin Treatment for Sleep Disorders in Parkinson’s Disease: A Meta-Analysis and Systematic Review. Front Aging Neurosci. 2022 Feb 4;14:784314. doi: 10.3389/fnagi.2022.784314. PMID: 35185525; PMCID: PMC8855052.
Kramer DJ, Johnson AA. Apigenin: a natural molecule at the intersection of sleep and aging. Front Nutr. 2024 Feb 27;11:1359176. doi: 10.3389/fnut.2024.1359176. PMID: 38476603; PMCID: PMC10929570.
Salehi B, Venditti A, Sharifi-Rad M, Kręgiel D, Sharifi-Rad J, Durazzo A, Lucarini M, Santini A, Souto EB, Novellino E, Antolak H, Azzini E, Setzer WN, Martins N. The Therapeutic Potential of Apigenin. Int J Mol Sci. 2019 Mar 15;20(6):1305. doi: 10.3390/ijms20061305. PMID: 30875872; PMCID: PMC6472148.
Ray S. The neuroprotective potential of magnesium in Parkinson’s disease. Magnes Res. 2024 Jun 1;36(4):69-81. doi: 10.1684/mrh.2024.0523. PMID: 38953416.
Zhang C, Hu Q, Li S, Dai F, Qian W, Hewlings S, Yan T, Wang Y. A Magtein®, Magnesium L-Threonate, -Based Formula Improves Brain Cognitive Functions in Healthy Chinese Adults. Nutrients. 2022 Dec 8;14(24):5235. doi: 10.3390/nu14245235. PMID: 36558392; PMCID: PMC9786204.
Mukherjee, S.; Banerjee, O.; Singh, S. Chapter 6 – The role of B vitamins in protecting mitochondrial function. In Molecular Nutrition and Mitochondria, Ostojic, S.M., Ed.; Academic Press: 2023; pp. 167-193.
Calderón-Ospina CA, Nava-Mesa MO. B Vitamins in the nervous system: Current knowledge of the biochemical modes of action and synergies of thiamine, pyridoxine, and cobalamin. CNS Neurosci Ther. 2020 Jan;26(1):5-13. doi: 10.1111/cns.13207. Epub 2019 Sep 6. PMID: 31490017; PMCID: PMC6930825.
Anjum I, Jaffery SS, Fayyaz M, Samoo Z, Anjum S. The Role of Vitamin D in Brain Health: A Mini Literature Review. Cureus. 2018 Jul 10;10(7):e2960. doi: 10.7759/cureus.2960. PMID: 30214848; PMCID: PMC6132681.
Małgorzata Mrowicka, Jerzy Mrowicki, Grzegorz Dragan, Ireneusz Majsterek; The importance of thiamine (vitamin B1) in humans. Biosci Rep 31 October 2023; 43 (10): BSR20230374. doi: https://doi.org/10.1042/BSR20230374
Williams PA, Harder JM, Foxworth NE, Cochran KE, Philip VM, Porciatti V, Smithies O, John SW. Vitamin B3 modulates mitochondrial vulnerability and prevents glaucoma in aged mice. Science. 2017 Feb 17;355(6326):756-760. doi: 10.1126/science.aal0092. PMID: 28209901; PMCID: PMC5408298.
Kannan K, Jain SK. Effect of vitamin B6 on oxygen radicals, mitochondrial membrane potential, and lipid peroxidation in H2O2-treated U937 monocytes. Free Radic Biol Med. 2004 Feb 15;36(4):423-8. doi: 10.1016/j.freeradbiomed.2003.09.012. PMID: 14975445.
Yuxiang Zheng, Lewis C. Cantley; Toward a better understanding of folate metabolism in health and disease. J Exp Med 4 February 2019; 216 (2): 253–266. doi: https://doi.org/10.1084/jem.20181965
Mukherjee, S.; Banerjee, O.; Singh, S. Chapter 6 – The role of B vitamins in protecting mitochondrial function. In Molecular Nutrition and Mitochondria, Ostojic, S.M., Ed.; Academic Press: 2023; pp. 167-193.
“Don’t let yourself be weighed down by what other people think, because in a few years, in a few decades, or in a few centuries, that way of thinking will have changed. Live now what others will only live in the future.” Paulo Coelho
Cover Photo Image by jacqueline macou from Pixabay

As usual, I learned a lot from reading this blog post. Very thorough, very well organized and very helpful. Loved the use of the schematics for delineating the many treatment options.
Many thanks Frank!
Bill
LikeLike
Thanks Bill, I appreciate your feedback. Sometimes, I spend more time preparing schematics and figures for a blog post than I do with the writing. Interestingly, I got the theme for the narrative portion of the blog {the first two sections) very quickly yesterday, the text flowed from my brain to the computer in less than an hour. By contrast, the two tables at the end took days and days to compile (searching, downloading, reading, writing, and editing); there was just no flow to them. Happy New Year Bill (the New Year blog post is in my head; I just need to make time to write), Frank
LikeLike
Dear Frank,
Thanks very much for your continuing sharing of information and insights. I have particularly appreciated your last two postings (Supplements for Treating Parkinson’s and The Year in Review).
Am I understanding correctly that your treatment strategy includes the daily use of carbidopa/levodopa IR 25mg/100mg tablets x 12 tablets/day? I ask this because I experienced some dyskinesia taking just 6 tablets each day (along with 200 mg of Entacapone 3 times per day). Are you experiencing any dyskinesia?
Best wishes for the New Year. I hope 2025 keeps your body healing healthy and strong and your soul soaring.
Michael
>
LikeLike
Michael,
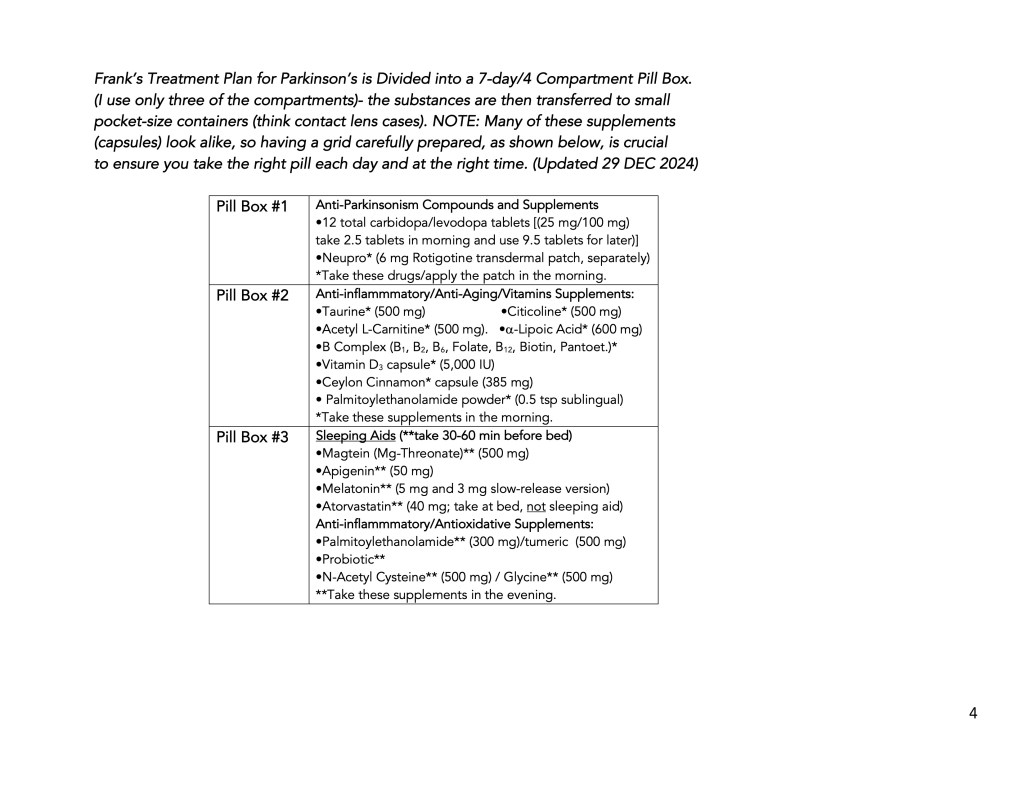
Thanks for the note. Yes, that is correct; I usually do 2.5 tablets at 7:00 AM, 2.5 tablets at 11:00 AM, 2.5 tablets at 3 PM, 2.5 tablets at 7 PM, and depending on how I feel when I get ready for sleep, I’ll take the final 2 tablets at 11 PM. I will stretch the timing for the late afternoon and early evening doses and frequently go 5 hrs between doses. And remember, I start out the morning with a 6 mg NeuPro dopamine agonist patch. Occasionally, I feel “totally off” in the morning, and I realize I have forgotten to trade out the old with a new DA patch. This dose of. carbidopa/levodopa IR and dopamine agonist patch have been carefully calibrated to be just the right amount for me. I have been taking carbidopa/levodopa for about 8 years (diagnosed in 2014, and the current dosing scheme since 2021. I have had no dyskinesia.
I, too, hope you have a healthy and happy 2025 and that you accomplish everything you have planned to do,
Frank
LikeLike
Thanks. Good to hear you are doing well.
Michael
LikeLike
Hello Frank! Thank you for sharing your journey, I really appreciate your experience and insight. I was wondering, have you tried L-theanine? What are your thoughts?
LikeLike
Chris,reverse insomna
thanks for your note. L-Theanine is popular right now, and I know some information about it, but not much. My interest in L-theonine is focused on its role in helping reverse sleep insomnia. However, when you read about, sure it can but it can cause vivid dreams/nightmares in living colr. Since I have already reached that point (I’ll have 1-2 of these colorful dreams per year without using L-theonine, then it made no sense to adding it. That is why I have a full body f it in my kitc
LikeLike
Chris, Let me start over. My intesret in L-theonine was for its ability to promote sleeping.However, vivid dreams is one of its side effects.Therefore, I decided that this was not something I needed in a sleeping tool box of supplements, so I’ve not used it. My sleeping aids include melatonin (5 mg regular release, and 3 mg slow release) apigenin (50 mg), and Magtein (Mg-theonate, 500 mg). Thanks for your note, bet wishes, Frank
LikeLike
THank you for sharing this information with us. The clear and orderly fashion you presented the data is also much appreciated.
My supplement regimen is similar to yours, with a few exceptions. I was diagnosed in 2023 and with good diet and exercise, I am doing quite well….for now. I have considered to start taking citicoline but I wanted to ask you if you had any positive or negative experiences with this supplement. Do you take it along with your morning CL dose?
Again, thanks for sharing your knowledge with us.
Marian
LikeLike
Hi Marian,
I apologize for the delayed response. Thanks for your positive comments about this blog post; they are really appreciated. Citicoline, yes, I have been taking it for almost a year. I take 500 mg in the morning. And I’ve got mixed feelings about whether it is working or not. There are definitely some nights when I get ready to take my final dose of carbidopa/levodopa that I’ve skipped a dose during the day. This would imply that I have generated either more dopamine or additional dopamine receptors, suggesting that citicoline is doing something. Then, many other days, I take my usual amount of carbidopa/levodopa with no change. The only difference between the days that I can tell or summarize is that when it doesn’t work I have been under some added stress, lack of sleep, or the day of much needed exercise. An alternative explanation is that I am further along with the global loss of dopamine receptors and that the machinery to respond to citicoline may be less efficient than someone with a newer disease (time-course wise). So I recommend trying citocoline and seeing if it reduces the amount of carbidopa/levodopa needed each day. Any reduction in carbidopa/levodopa would be a good thing. I will try to better track my carbidopa/levodopa daily consumption and add a review of citicoline to my list of future topics to write about. Best wishes, Frank
LikeLike
THank you, Frank!
I just received my shipment of citicoline and intend to start tomorrow. I’ll send you an update of my experience perhaps after 6-8 weeks of use.
By the way, did you experience any negative reaction or did you tolerate it well? I have read t hat many will experience some nausea, etc.
Again, thank you for your detailed response and wonderful column!
Best,
Marian
LikeLike
Marian, I have had no side effects from using Citicoline, no nausea. I hope it has a positive impact on your carbidopa-levodopa levels. Thanks for the update, Frank
LikeLike