


“Being happy doesn’t mean that everything is perfect. It means that you’ve decided to look beyond the imperfections.” Gerard Way
“Rules for Happiness: something to do, someone to love, something to hope for.” Immanuel Kant
Introduction: I have a new friend with Parkinson’s. He has always been very active and genuinely enjoys playing golf. However, he has a hard time controlling dystonia, which has hindered much of his daily exercise. This got me thinking, and it leads me to the topic of this blog post. The goal is to describe how botulinum toxin works, allowing someone with Parkinson’s and bothersome dystonia some regular relief. Botulinum toxin is also used to treat excessive drooling (sialorrhea) and even the Parkinson’s tremor in some clinical studies.
“If you want to live a happy life, tie it to a goal, not to people or objects.” Albert Einstein
A Primer on Botulinum Toxin: Botulinum toxin, abbreviated as BTX or BoNT, is derived from the anaerobic bacteria, Clostridium botulinum. Anaerobic? This refers to an organism that is capable of living and existing in the absence of free oxygen. Humans are aerobic organisms; we definitely need oxygen to survive. There are seven neurotoxins from BTX, designated A, B, C (C1, C2), D, E, F, and G. The most widely used BTX is Botox® (OnabotulinumtoxinA).The BTX substance is a protease, a protein that cleaves or chews-up other proteins. BTX is a two-chain (heavy and light) zinc-containing metalloprotease. The heavy chain gives the cholinergic specificity (help direct binding to presynaptic receptors), the light chain has the proteolytic activity.
BTX mode of action is binding presynaptically to high-affinity sites on nerve terminals, which ultimately stops the release of acetylcholine, causing paralysis of the neuromuscular effect. The mechanism that has been worked out for BTX is as follows: (i) the light chain BTX recognizes and cleaves SNARE proteins (SNAP-25, Syntaxin, Synaptobevin), (ii) typically, these SNARE proteins form a complex with neurotransmitters and are contained in vesicles, (iii) cleaved SNARE proteins do not complex with acetylcholine; (iv) the fusion of membranes does not occur; (v) acetylcholine is not released into the muscle cell; thus, paralyzing the cell. (vi) Over time, the neuromuscular junction regenerates as the activity (life-time) of BTX diminishes. The drawing below explains the process of how BTX works.

“Success is not the key to happiness. Happiness is the key to success. If you love what you are doing, you will be successful.” Albert Schweitzer
Therapeutic Uses and Cosmetic Purposes for BTX: Keeping in mind that BTX is one of the most poisonous biological substances known, it has found wide use in both the medical world and in the setting of cosmetic treatment. By blocking the release of acetylcholine in the neuromuscular junction, BTX causes temporary paralysis of the muscle. Depending on where the BTX has been injected, this temporary paralysis can last 3-6 months. BTX injection has been used for treating several medical conditions, including: strabismus (abnormal alignment of the eyes such as someone with squinting eyes), focal dystonias (involuntary spasms in small muscles in the body), hemifacial spasm [frequent involuntary contractions (spasms) of the muscles on one side (Hemi-) of the face (facial)], migraine headaches, hypersalivation, and hyperhidrosis (abnormally excessive sweating). This is but a brief list of some of the various conditions treated with BTX. In the world of cosmetics, BTX has found a lot of use in reducing facial wrinkles, lines, and creases.
The FDA in the USA has approved the following BTX products and for the following uses (derived and compiled from “Manufacture of Commercial Botulinum Neurotoxins for Human Treatment” by E.A. Johnson and neuromuscular-blockers-botulinum-toxins from Medscape):
–OnabotulinumtoxinA (Botox®, Botox Cosmetic®),
Botox® – Cervical dystonia, severe primary axillary hyperhidrosis, strabismus, blepharospasm, neurogenic detrusor overactivity, chronic migraine, upper limb spasticity
Botox Cosmetic® – Moderate to severe glabellar lines, moderate to severe lateral canthal lines, known as crow’s feet
–AbobotulinumtoxinA (Dysport®) – Upper and lower limb spasticity, cervical dystonia, and moderate-to-severe glabellar lines in adults; it is also indicated for lower limb spasticity in children aged 2 years or older
–IncobotulinumtoxinA (Xeomin®) – Upper limb spasticity, cervical dystonia, blepharospasm, moderate to severe glabellar lines, chronic sialorrhea
-PrabotulinumtoxinA (Jeuveau®) – Moderate-to-severe glabellar lines
-RimabotulinumtoxinB (Myobloc®) – Cervical dystonia
Given at the end of the post are some references/literature for anyone interested in the original study/review.
“The happiness of your life depends upon the quality of your thoughts.” Marcus Aurelius
BTX for Treating Dystonia in Parkinson’s: Dystonia is an abnormal muscle tone that leads to muscular spasm and abnormal posture. Dystonia usually occurs due to either neurological disease or a side effect of drug therapy. Carbidopa/Levodopa treatment can have a variable response to dystonia, improving it, or making it worse in some people-with-Parkinson’s (PwP).
Dystonia on its own is a movement disorder, and it occupies the number three slot in terms of the number of cases of movement disorders. Dystonia is a frequent component of Parkinson’s. It is estimated that between 50-60% of PwP have some first-hand experience with dystonia.
BTX has been shown in several clinical studies to improve painful foot dystonia. Typically, BTX was injected into two muscles based on the resulting shape of the toes/foot. However, other studies were met with less success. One can imagine this variable-type of response is due to the location of the affected muscle(s) in hand or foot and the precise anatomic location chosen for injection of the BTX into the muscle. The figure below highlights some of the aspects of dystonia in Parkinson’s and many possible muscles available for injecting and directing the BTX to remove the affected muscle’s pain and frustration.

“The most important thing is to enjoy your life – to be happy – it’s all that matters.” Audrey Hepburn
BTX for Treating Sialorrhea (Drooling) in Parkinson’s: Drooling or excess saliva is commonly found in Parkinson’s. It is thought that the PwP with sialorrhea does not have increased production of saliva, but it is due to a dysfunction of salivary function or clearance (e.g., one does not swallow enough to clear out the saliva). Reducing the amount of saliva produced by temporarily halting its release from the salivary gland by BTX treatment could provide relief from the ‘burden’ of getting rid of excess. Drooling in Parkinson’s is quite common, occurring >70% in PwP.
There have been several clinical trials done with BTX to control drooling in PwP, and they have all met with some success (when compared to controls). Evidently, most studies have focused on the parotid gland to target neuromuscular junctions with BTX to temporarily paralyze these muscles to reduce the overall burden for saliva. Given below in the figure are examples of anatomic components in the mouth that are likely targets for BTX treatment to control sialorrhea in Parkinson’s.

“Happiness is not a goal; it is a by-product.” Eleanor Roosevelt
BTX for Treating Tremor in Parkinson’s: The Parkinson’s tremor is one of the disorder’s “Cardinal features”, but not everyone has this tremor. The Parkinson’s tremor in some PwP can be well-controlled with Carbidopa/Levodopa, but it does not work nearly as well in others. Thus, it’s more of a nuisance for most people, but with time people will explore deep brain stimulation surgery, for example, the potential use of BTX.
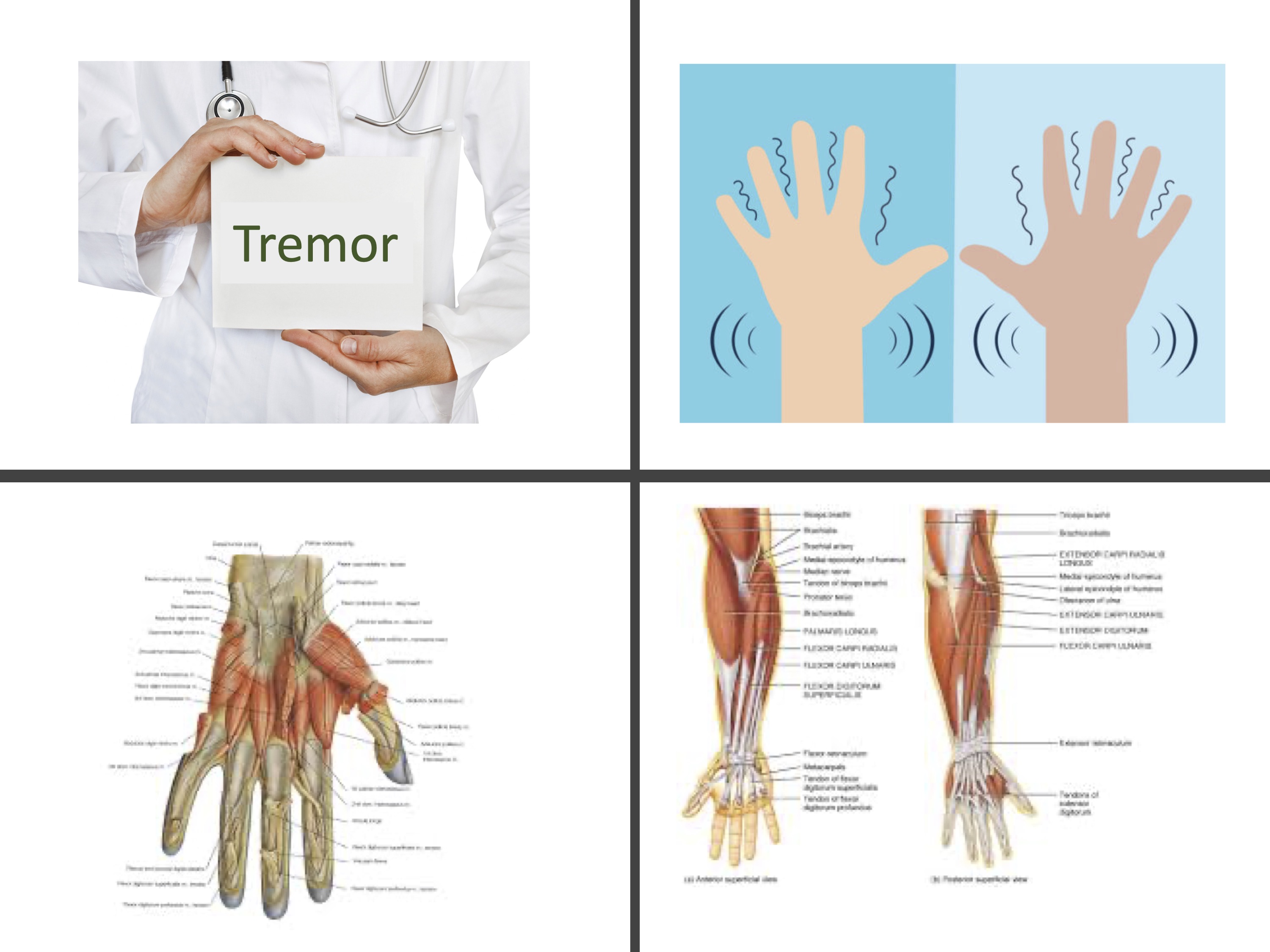
There have been many different clinical trials using BTX to safely treat the hand tremor in Parkinson’s. Typically, based on the numbers of patients, this is merged with others with essential tremor. In one of the earlier studies from 1991, using 51 patients, injecting BTX into the forearm extensor and flexor muscles. The study showed some improvement in the tremor group compared to controls. The only negative result noted was occasional focal muscle weakness.
In a different clinical study to evaluate BTX and Parkinson’s tremor, the BTX injection was guided using electromyographic (EMG) technology to optimize the toxin’s effect on muscle. In trying to summarize the results published, it would appear that BTX in tremor is much more complicated to achieving success due to a large number of muscle injection sites that are typically required. By contrast, the fewer muscles involved in dystonia have shown that BTX has been much more successful. Shown below are the numerous muscles in the forearm and hand, which suggest that achieving success with BTX to manage tremor can be a difficult process.
“The secret of happiness is not in doing what one likes, but in liking what one does.” James M. Barrie
BTX and Treating Parkinson’s: In this blog post, I have tried to summarize the use of BTX in treating various symptoms of Parkinson’s. During my education, it became apparent that BTX may have some real application in certain parts of Parkinson’s, but not all aspects of this disorder. Remembering that I am a scientist, not a clinician, and I’m not recommending anyone try any of these techniques clinically without first consulting your neurologist and your family. However, these are interesting scientific observations. BTX is found wide application in medicine, attending many different sorts of problems in patients, met with much success. I have only mentioned a few of the applications of BTX and Parkinson’s, primarily because the process is precisely the same using small amounts of BTX are injected into neuromuscular junctions. Cited below are 12 different journal articles; some are review articles. Some are primary clinical trial studies and will give you much more depth and detail into the use of BTX in Parkinson’s.
“Be so happy that when others look at you, they become happy too.” Harbhajan Singh Yogi
References for Botulinum Toxin and Parkinson’s disease:
- Mills, R., Bahroo, L. and Pagan, F., 2015. An update on the use of botulinum toxin therapy in Parkinson’s disease. Current neurology and neuroscience reports, 15(1), p.511.
- Dogu, O., Apaydin, D., Sevim, S., Talas, D.U. and Aral, M., 2004. Ultrasound-guided versus ‘blind’intraparotid injections of botulinum toxin-A for the treatment of sialorrhoea in patients with Parkinson’s disease. Clinical neurology and neurosurgery, 106(2), pp.93-96.
- Sheffield, J.K. and Jankovic, J., 2007. Botulinum toxin in the treatment of tremors, dystonias, sialorrhea and other symptoms associated with Parkinson’s disease. Expert Review of Neurotherapeutics, 7(6), pp.637-647.
- Ruiz-Roca, J.A., Pons-Fuster, E. and Lopez-Jornet, P., 2019. Effectiveness of the botulinum toxin for treating sialorrhea in patients with Parkinson’s disease: a systematic review. Journal of Clinical Medicine, 8(3), p.317.
- Cardoso, F., 2018. Botulinum toxin in parkinsonism: The when, how, and which for botulinum toxin injections. Toxicon, 147, pp.107-110
- Pacchetti, C., Albani, G., Martignoni, E., Godi, L., Alfonsi, E. and Nappi, G., 1995. “Off” painful dystonia in Parkinson’s disease treated with botulinum toxin. Movement disorders: official journal of the Movement Disorder Society, 10(3), pp.333-336.
- Jankovic, J., 2009. Disease-oriented approach to botulinum toxin use. Toxicon, 54(5), pp.614-623.
- Shetty, A.S., Bhatia, K.P. and Lang, A.E., 2019. Dystonia and Parkinson’s disease: What is the relationship?. Neurobiology of disease, 132Niemann, N. and Jankovic, J., 2018. Botulinum toxin for the treatment of hand tremor. Toxins, 10(7), p.299.
- Gupta, A.D. and Visvanathan, R., 2016. Botulinum toxin for foot dystonia in patients with Parkinson’s disease having deep brain stimulation: a case series and a pilot study. Journal of Rehabilitation Medicine, 48(6), pp.559-563.
- Samotus, O., Lee, J. and Jog, M., 2020. Standardized algorithm for muscle selection anddosing of botulinum toxin for Parkinson tremor using kinematic analysis. Therapeutic advances in neurological disorders, 13, p.1756286420954083.
- Wree, A., Hawlitschka, A., Holzmann, C., Witt, M., Kurth, J., Lindner, T., Mann, T. and Antipova, V., 2020. Interlinking potential therapy with botulinum neurotoxin-A and Parkinson’s disease. In Diagnosis and Management in Parkinson’s Disease (pp. 665-681). Academic Press.
- Lagalla, G., Millevolte, M., Capecci, M., Provinciali, L. and Ceravolo, M.G., 2006. Botulinum toxin type A for drooling in Parkinson’s disease: a double‐blind, randomized, placebo‐controlled study. Movement disorders: official journal of the Movement Disorder Society, 21(5), pp.704-707.
“Learn to enjoy every minute of your life. Be happy now. Don’t wait for something outside of yourself to make you happy in the future. Think how really precious is the time you have to spend, whether it’s at work or with your family. Every minute should be enjoyed and savored.” Earl Nightingale
Cover image by Antonios Ntoumas from Pixabay
