


“Apathy is the acceptance of the unacceptable.” John Stott
“I don’t know, I don’t care, and it doesn’t make any difference.” Jack Kerouac
Definition: Apathy (ap·a·thy, /ˈapəTHē/) lack of interest, enthusiasm, or concern.
Occurrence of Apathy in Parkinson’s: The presence of apathy in Parkinson’s is between 17% to 70%, the wide range is partly due to the imprecise clinical definition of apathy.
A Personal Story: For the past few months, I have been feeling lazy, non-compliant regarding exercise, and just lacking the drive and commitment that I felt I needed to thrive in the presence of Parkinson’s. But here is the problem, I started believing it, started denying everything that should reverse this feeling. Over time, I began to feel it was the path to follow. But, I then reached a point and thought to myself, “Damn it, Frank, get up, get going, get your brain-in-the-game, let’s go, and keep going. Do it now!” And things began to change with this renewed focus. However, this was either my first-time experience with apathy or a side-effect of my dopamine agonist withdrawal that promoted apathy? Regardless, I did not like it at all. So, let me start first with a description of apathy.
“Is it ignorance or apathy? Hey, I don’t know and I don’t care.” Jimmy Buffett
The Clinical Explanation: Pluck and Brown (2002) described apathy this way, “Apathy refers to a constellation of behavioural, emotional, and motivational features including a reduced interest and participation in normal purposeful behaviour, lack of initiative with problems in initiation or sustaining an activity to completion, lack of concern or indifference, and a flattening of affect.” Furthermore, they go on to say, “Almost by definition, apathy has a direct impact on the overall level of handicap, as it reduces participation in age appropriate activities above and beyond that due to other aspects of the disease.” To read this open access paper, Pluck, G. C., and R. G. Brown. “Apathy in Parkinson’s disease.” Journal of Neurology, Neurosurgery & Psychiatry 73.6 (2002): 636-642, click here.
In an attempt to further describe apathy, Pagonabarraga et al. (2015) said, “Motivation is a psychological feature that arouses an organism to act towards a desired goal, both eliciting and sustaining goal-directed behaviours.12 Motivation in healthy human beings acts as an inner drive elicited by physical needs (e.g., eating and drinking), but also by pleasurable and aversive stimuli, as coded by reward-based and punishment-based learning, which attach motivational importance to otherwise neutral environmental stimuli. 1“ Click here to see this reference, Pagonabarraga, J., Kulisevsky, J., Strafella, A. P., & Krack, P. (2015). Apathy in Parkinson’s disease: Clinical features, neural substrates, diagnosis, and treatment. The Lancet Neurology, 14(5), 518-531. doi:http://dx.doi.org.libproxy.lib.unc.edu/10.1016/S1474-4422(15)00019-8
“The wise man does at once what the fool does finally.” Niccolo Machiavelli
Describing the Difference Between Depression, Anxiety, and Apathy in Parkinson’s: If one is being considered for apathy, the physician must clearly distinguish apathy from depression, since they can be related to one another in Parkinson’s. However, the symptoms of depression can normally be distinguished from apathy, when one compares the symptoms listed below. And while anxiety is quite common in Parkinson’s, it seems less linked to apathy; however, some studies have anxiety and apathy somewhat clustered together.
- Some of the Symptoms of Apathy include reduced initiative, decreased participation in external activities unless engaged by another person, loss of interest in social events or everyday activities, decreased interest in the world around him or her, emotional indifference, less affection than usual, lack of concern for others’ feelings/interests.
- Some of the Symptoms of Depression include sadness, feeling of guilt, negative thoughts/feelings, helplessness, hopelessness, pessimissm, self-criticism, anxiety, suicidal ideation.
- Some Overlapping Symptoms of Apathy and Depression include psychomotor retardation, anhedonia (Inability to feel pleasure), anergia (abnormal lack of energy), less physical activity than usual, decreased enthusiasm for usual interests.
- Some of the Typical Symptoms of Anxiety include feeling nervous, restless or tense, sense of impending danger, panic or doom, increased heart rate, breathing rapidly (hyperventilation), feeling weak or tired, difficulty in concentrating or thinking about anything other than the present worry (“hypervigilance”).
- From these list of symptoms, I can see the relationship linking apathy to depression but much less so for apathy too anxiety.
“Apathy is one of the characteristic responses of any living organism when it is subjected to stimuli too intense or too complicated to cope with. The cure for apathy is comprehension.” John Dos Passos
Defining and Identifying Apathy: Marin and Levy and Dubois defined apathy “as a state of decreased motivation that presents itself as a reduction in goal-directed behavior, and further described as someone with reduced interests (or emotions) that cannot be attributed to lessened consciousness, cognitive impairment, or emotional distress.”
Psychologists use the term subdomain to identify discrete neural components that add up to characterize someone with either a cognitive or a behavioral syndrome. Apathy is linked to four subdomains including (1) reward deficiency syndrome (reduction in emotional stability), (2) executive dysfunction (decreased cognitive interests), (3) auto-activation deficiency (reduced spontaneous use of mental processes), and (4) depression. The sum of these subdomains describe apathy; however, one could imagine the contribution of each subdomain vary from one patient to the next. Knowledge of the contribution from each subdomain helps the physician design an individualized treatment plan for someone with apathy.
Driving these subdomains are neural circuits, and defective/altered circuitry is found in neurodegenerative disorders like Parkinson’s. A short overview of some of the neural circuits is next.
“Apathy can be overcome by enthusiasm.” Arnold J. Toynbee
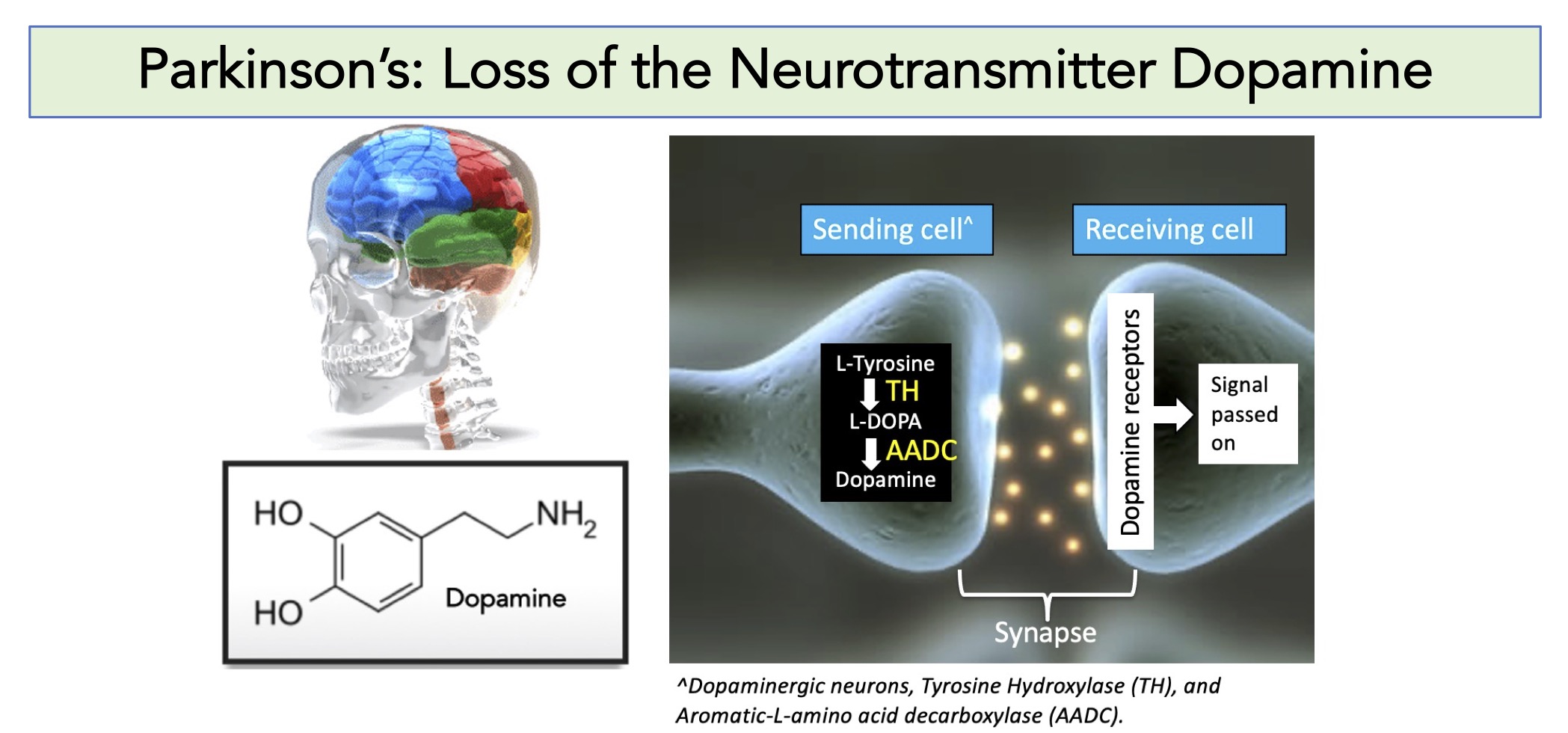
Dopamine Pathways in the Brain: Dopamine is a neurotransmitter synthesized in the substantia nigra pars compacta. Interesting, dopamine is involved in 4 different pathways in the brain, as briefly described below:
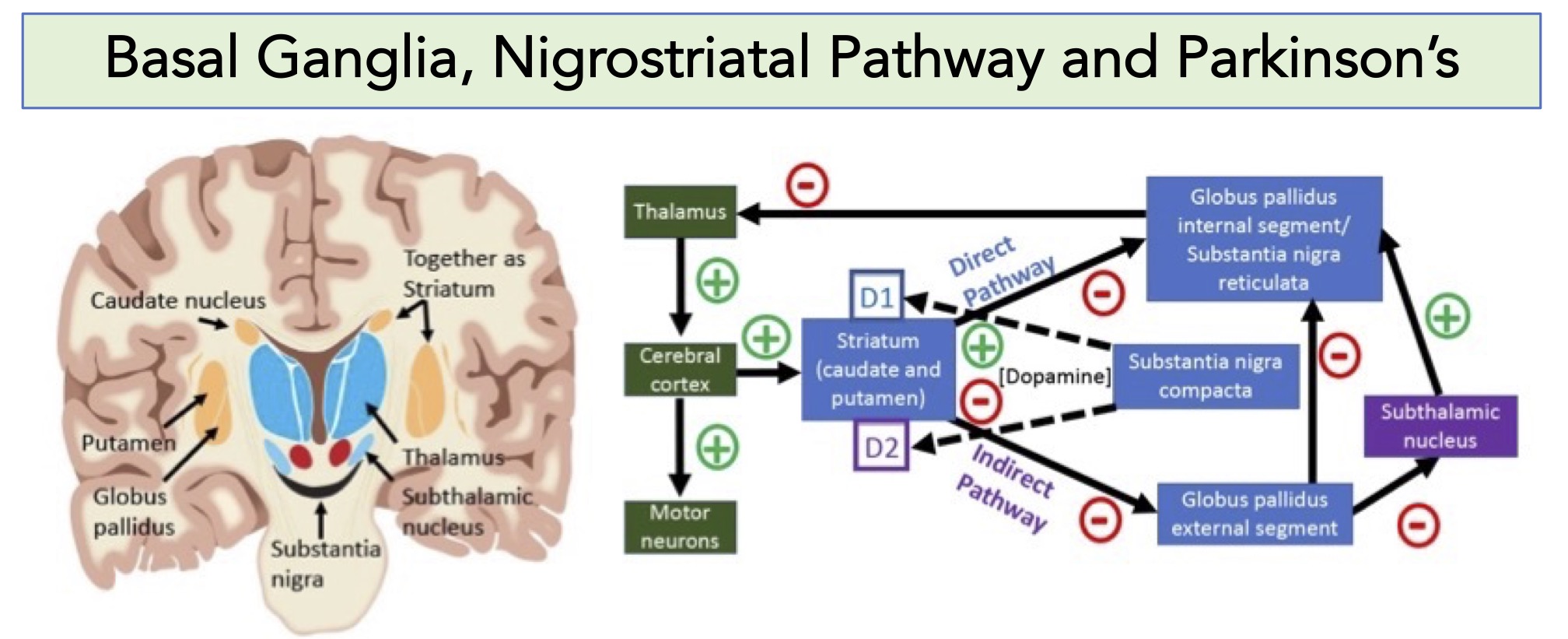
- Nigrostriatal Pathway: The nigrostriatal pathway is a bilateral dopaminergic pathway in that connects the substantia nigra pars compacta (SNc) in the midbrain with the dorsal striatum (i.e., the caudate nucleus and putamen) in the forebrain. The nigrostriatal pathway is involved in motor function; >75% of the dopamine sythesized in the brain is used in this pathway. Please see the figure below where this pathway is partly explained.
- Mesocortical Pathway: Projections from the ventral tegmental area to prefrontal cortex. Responsible for behavioral/executive function. The mesocortical pathway uses dopamine to help direct our memory, focus, and decision-making. Please see the figure below where this pathway is partly explained.
- Mesolimbic Pathway: Projections from the ventral tegmental area to forebrain (especially the nucleus accumbens in the basal forebrain). Responsible for emotional function. The mesolimbic pathway is associated with dopamine’s function related to reward and pleasure. Please see the figure below where this pathway is partly explained.
- Tuberoinfundibular Pathway: Projections from the hypothalamus to the pituitary gland. The origins of the pathway are classically assigned to the periventricular and arcuate (infundibular) nuclei. The tuberoinfundibular pathway uses dopamine to inhibit prolactin release in the pituitary system, which can stimulate breast milk production.
“Science may have found a cure for most evils; but it has found no remedy for the worst of them all – the apathy of human beings.” Helen Keller
The Pathways of the Brain that Predispose One to Apathy, Motivation, and Emotions: If you have read this far, you must be realizing, wow, the brain is really complicated and it does so much. Writing this post makes my brain hurt from trying to understand it well enough to try to write about it. However, the simple answer is that the depth of what the brain is capable of doing is beyond easy description and it really requires a lot of effort to understand its function. Nonetheless, here are some pictures/schematics to try to decipher how apathy results because of Parkinson’s, and in most cases, direct lesions or damage to specific brain regions:
- Much of this work is based on studies of people following strokes and having motivation issues; specifically, they had brain lesions that were mapped to areas involved in brain regions that controlled emotion and motivation.
- Of importance included the basal ganglia [specifically, the ventral parts, the globus pallidus and ventral striatum (vStr)], the anterior cingulate cortex (ACC), and the ventromedial prefrontal cortex (vmPFC, and it is also called the medial orbitofrontal cortex or OFC).
- In surgery of psychiatric patients, pleasure was found linked to the nucleus accumbens (NAc) and the ventral pallidum.
- In animal studies, motivation was clearly linked to the ventral basal ganglia structures (NAc and ventral pallidum), ACC, ventral tegmental area (VTA) and the basolateral amygdala (BLA).
- Importantly, as mentioned in the section above, the VTA is responsible for providing dopamine projections to the vStr (referred to as the mesolimbic dopamine pathway), and the PFC (the mesocortical dopamine pathway), and then to the amygdala.
- Dopamine is clearly involved in these circuits, but other neurotransmitter systems also have a role.
- Since dopamine deficiency is clearly a hallmark in Parkinson’s, apathy can be found in all stages of the disorder.
- Imagining studies in Parkinson’s patients have implicated the ventral striatum (VStr), anterior cingulate cortex (ACC) and regions of the prefrontal cortex connected with the midbrain dopamine-containing ventral tegmental area (VTA).
- Dopamine depletion in Parkinson’s is not uniform in the striatum, which suggests that expression of apathy may differ from person to person depending on which ‘region’ of the brain has received the least amount of dopamine.
- The top panel of the figure below just reminds one of the structure of dopamine and the neurotransmitter function of neurons sending and receiving dopamine.
- The middle panel of the figure below reviews the motor function of dopamine through the nigrostriatal pathway.
- The bottom panel of the figure is derived from two papers that are described in the legend below. The left side of the bottom panel highlights the regions of the brain that control social behavior and emotion, while the right side of the bottom panel highlights the circuits that wire these regions of the brain together, this includes the mesocortical and the mesolimbic pathways of dopamine. [You can enlarge the top, middle, and bottom portions of these images by clicking on them.]

“Willpower is the key to success. Successful people strive no matter what they feel by applying their will to overcome apathy, doubt or fear.” Dan Millman
Dopamine Agonist Withdrawal Syndrome and Apathy: Most of you know I recently ‘stopped’ using Ropinirole, a dopamine agonist. The protocol went from 18 mg/day to 0 mg/day in about 3-4 weeks, which is rapid. One can imagine that excess dopamine (given here as a dopamine agonist) could result in behavioral changes and addiction patterns (Impulse control disorders). The opposite, leading to a state of a hypodopaminergic syndrome (removal of dopamine agonist), could result in apathy, anxiety, and depression, which describes DAWS or dopamine agonist withdrawal syndrome.
After talking it over with my Neurologist, he agrees that the sudden drop of the dopamine agonist likely led to me being somewhat numb or apathetic. My realization was a positive key and step to reversing the ‘feeling.’ I successfully removed Ropinirole from my daily medical chest. However, there was some residual, let’s say, like a ‘prolonged hangover’ that left me with apathy. Alternatively, maybe this is the ‘ground state’ that I am supposed to be at in a more normal feeling. Especially since the feeling of being wired and always on is gone following the dopamine agonist taper down.
In conclusion, I have learned a lot from this blog post. For example, the importance of dopamine in apathy, distinguishing apathy, depression, and anxiety, and the occurrence of apathy in Parkinson’s. There was so much material that could have (maybe should have been) included here. Below is a list of references used in my preparation for this blog post; you may learn a lot by reading over these papers (they are fascinating). Stay healthy all.
“Some people confuse acceptance with apathy, but there’s all the difference in the world. Apathy fails to distinguish between what can and what cannot be helped; acceptance makes that distinction. Apathy paralyzes the will- to- action; acceptance frees it by relieving it of impossible burdens.” Arthur Gordon Webster
Cover photo Image by sabri ismail from Pixabay
References for this blog post (a Google Scholar survey lists >30,000 publications when using the key words, “Apathy and Parkinson’s disease”):
Pluck, G.C. and Brown, R.G., 2002. Apathy in Parkinson’s disease. Journal of Neurology, Neurosurgery & Psychiatry, 73(6), pp.636-642.
Pagonabarraga, J., Kulisevsky, J., Strafella, A.P. and Krack, P., 2015. Apathy in Parkinson’s disease: clinical features, neural substrates, diagnosis, and treatment. The Lancet Neurology, 14(5), pp.518-531.
Levy, R. and Dubois, B., 2006. Apathy and the functional anatomy of the prefrontal cortex–basal ganglia circuits. Cerebral cortex, 16(7), pp.916-928.
Husain, M. and Roiser, J.P., 2018. Neuroscience of apathy and anhedonia: a transdiagnostic approach. Nature Reviews Neuroscience, 19(8), pp.470-484.
Le Heron, C., Apps, M.A.J. and Husain, M., 2018. The anatomy of apathy: a neurocognitive framework for amotivated behaviour. Neuropsychologia, 118, pp.54-67.
Le Heron, C., Holroyd, C.B., Salamone, J. and Husain, M., 2019. Brain mechanisms underlying apathy. Journal of Neurology, Neurosurgery & Psychiatry, 90(3), pp.302-312.
Mele, B., Van, S., Holroyd-Leduc, J., Ismail, Z., Pringsheim, T. and Goodarzi, Z., 2020. Diagnosis, treatment and management of apathy in Parkinson’s disease: a scoping review. BMJ open, 10(9), p.e037632.
Sherwin, E., Bordenstein, S.R., Quinn, J.L., Dinan, T.G. and Cryan, J.F., 2019. Microbiota and the social brain. Science, 366(6465).
