


“Resilience is accepting your new reality, even if it’s less good than the one you had before.” Elizabeth Edwards
“Health is wholeness and balance, an inner resilience that allows you to meet the demands of living without being overwhelmed.” Andrew Weil
Introduction: The goal is to review the role(s) played by dopamine, serotonin, norepinephrine (also called noradrenaline), and acetylcholine in Parkinson’s. The easy part of understanding Parkinson’s is motor dysfunction and how important dopamine is for this disorder. By contrast, what role does this loss of dopamine and its interactions with other neurotransmitter systems has to do with the non-motor features of Parkinson’s is where it gets confusing to me and, likely, many others. I keep going back and reading many articles, but I still lack clarity.
Thus, my attempt here is to continue educating me (and hopefully you) on the importance of neurotransmitters in our brains. Are you constipated, feeling down, not sleeping well, freezing of gait, having psychotic tendencies, cognitive decline, or having difficulty focusing? This blog post may not fully answer these questions. Still, hopefully, it will give you an appreciation of neurotransmitters and their roles in explaining motor and non-motor defects.
“The ability to take misfortune and make something good come of it is a rare gift. Those who possess it are ..said to have resilience or courage.” Mihaly Csikszentmihalyi
Pathophysiology and Progression of Parkinson’s:
•Parkinson’s evolves from the death of dopaminergic neurons in the substantia nigra pars compacta.
•The lesion that causes neuronal cell death is named the Lewy body, an aggregated clump (denatured and insoluble) of material containing mainly the protein called a-synuclein.
•The most accepted model of how Parkinson’s starts is the Braak model, which suggests the disorder originates in the olfactory bulb and medulla. These symptoms relate to sleep dysfunction and loss of smell before developing motor symptoms.
•As these lesions progress, the substantia nigra and other midbrain regions and some forebrain become affected, and the motor symptoms evolve. It is at this stage the diagnosis of Parkinson’s is usually made.
•Lesions continue throughout the brain, leading to cerebral cortices dysfunction, whereby cognitive issues could arise, and dementia or hallucinations could occur.
• Parkinson’s is traditionally defined as a movement disorder; we use dopamine precursors, dopamine mimics, or substances that preserve endogenous dopamine as critical therapeutics. For most of us, there is a viable treatment.
•However, we also now understand that other neurotransmitter systems are modified in Parkinson’s.
•These changes to the neurotransmitters’ properties partly explain why some symptoms of Parkinson’s do not respond to dopamine replacement treatment.
“The key to life is resilience….We will always be knocked down. It’s the getting up that counts.” Dominique Browning
What are Neurotransmitters? The Cleveland Clinic describes neurotransmitters as follows: “Neurotransmitters are your body’s chemical messengers. They carry messages from one nerve cell across a space to the next nerve, muscle or gland cell. These messages help you move your limbs, feel sensations, keep your heart beating, and take in and respond to all information your body receives from other internal parts of your body and your environment.”
Dopamine, Serotonin, Norepinephrine (also called Noradrenaline), and Acetylcholine– There are many neurotransmitters performing their work every minute we live. The four here have some overlapping areas of interest in their regulatory roles, yet they are compelling. Given in Table 1 below are these neurotransmitters, their primary site(s) of synthesis in the brain, and their biological roles. Below the Table is the simple yet elegant structures for each compound.
“Man never made any material as resilient as the human spirit.” Bernard Williams
Parkinson’s is a Complex Disorder: We have learned much about Parkinson’s over the years. First, we know that it is a very heterogeneous disorder. This implies that it is more complex than just the loss of dopaminergic neurons in the substantia nigra pars compacta. Many people with Parkinson’s will have much more than just the Cardinal signs of Parkinson’s related to motor functions, that is, rigidity, bradykinesia, postural instability, and tremor. In addition, we now have a cadre of non-motor symptoms, such as depression, psychosis, dementia, hyposmia (decreased sense of smell), rapid eye movement (REM) sleep behavior disorder, and constipation.
Thus, Parkinson’s is a complicated disorder that evolves due to the disruption and dysfunction of several pathways, gene modulation, and the environment all coming together to produce this disease. As mentioned above, this post is focused on dopamine and dopamine’s connection with serotonin, norepinephrine (also called noradrenaline), and acetylcholine and their role in Parkinson’s. We continue the story with dopamine.
“The best antidote to stress is resilience… having the ability to respond to change or adversity proactively and resourcefully.” Lauren Mackler
Dopamine Depletion: We have a supply and demand problem in Parkinson’s, given that our dopamine tank is depleted, and we are managing life with a reduced dopamine load. And we are continually adding back to our diminishing tank of dopamine by taking drugs (Sinemet and levodopa-based substances, dopamine agonists, and the like), exercising, and trying to sleep more and better. In addition, many are trying a Complementary & Alternative Medicine (CAM) approach to keep our remaining dopaminergic neurons alive and working by attempting to halt or at least slow disease progression. So our task is multi-fold as we are challenged with a brain on 50% or less dopamine production than we had before Parkinson’s.
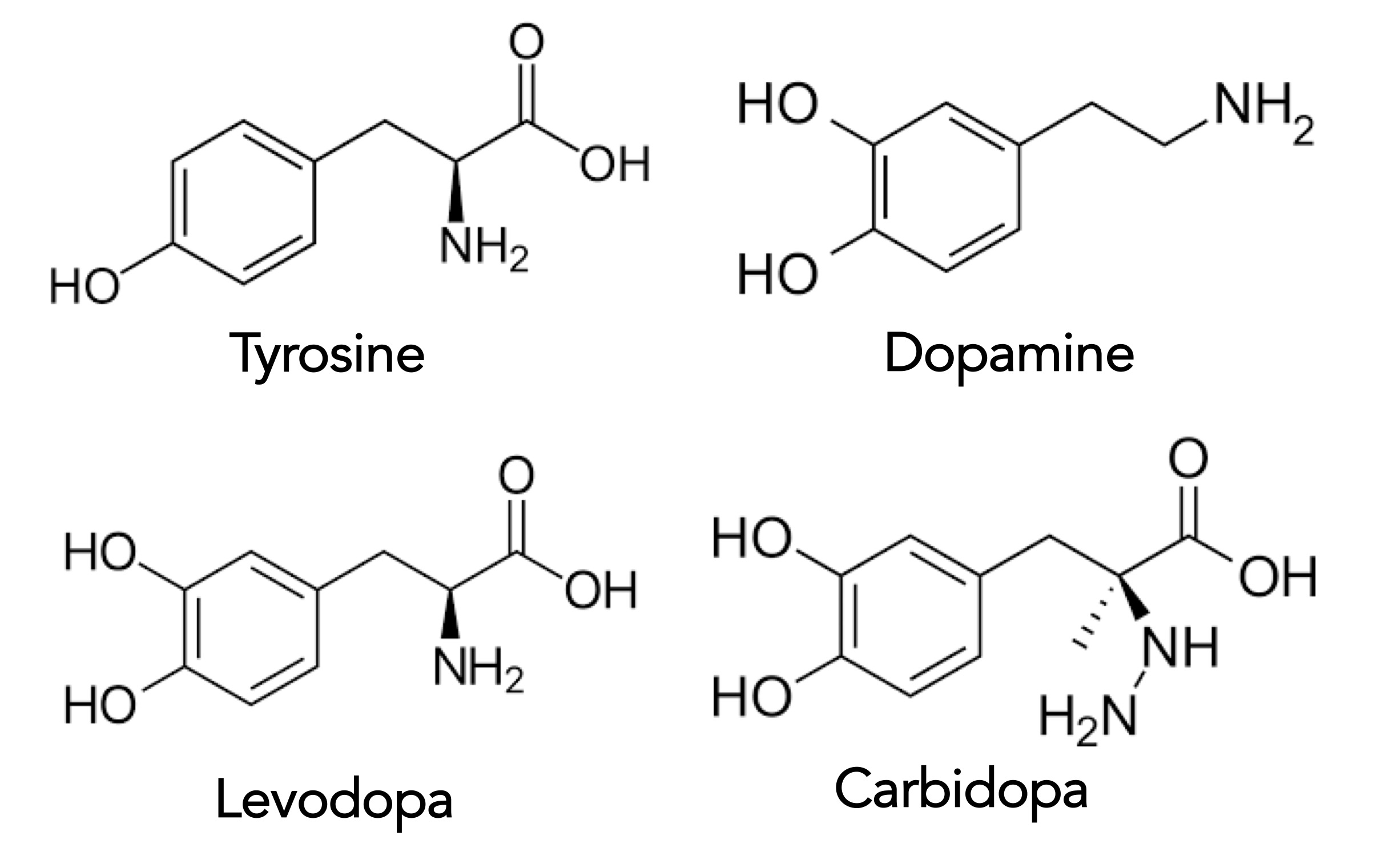
And the brain, oh yes, the beautiful brain, prevents exogenous dopamine from entering its space through the resistant blood-brain barrier. Look at the drawing below, where dopamine structures are compared to its precursor molecule, levodopa, and its protector molecule, carbidopa. The blood-brain barrier allows levodopa to pass into the brain, but neither the neurotransmitter in dopamine nor carbidopa, the tissue inhibitor that allows levodopa to pass through the bloodstream, are allowed to enter.
“Human beings have enormous resilience.” Muhammad Yunus
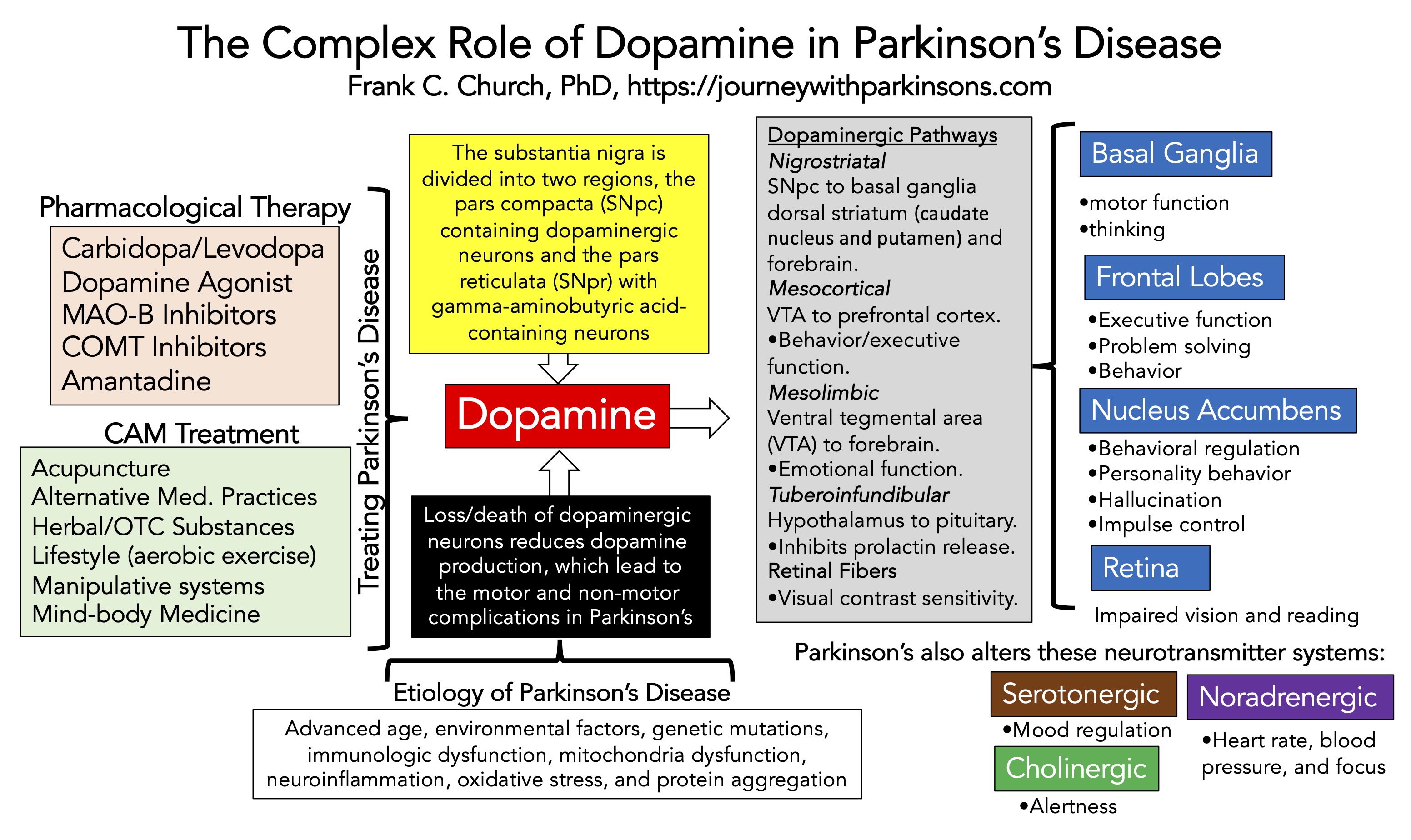
Dopamine Connections: Dopamine is needed in both motor- and non-motor-dependent events. The wonder of dopamine is given in the schematic below, followed by a brief overview of the significant pathways. The drawing is my attempt to summarize Parkinson’s in 1-page, focusing on the role of dopamine, the development of the disorder, physiological paths to function, and the various treatment modalities. The story gets complicated (and a bit murky) because besides dopaminergic neurons dying, there is evidence that other neurotransmitter systems are also diminishing. Thus, these neurotransmitter systems could contribute to both the motor- and non-motor complications of Parkinson’s.
“Resilience is based on compassion for ourselves as well as compassion for others” Sharon Salzberg
Dopaminergic Pathways:
Nigrostriatal Pathway- The pars compacta region of the substantia nigra is the primary producer of dopamine in the brain (makes 75-80%). The nigrostriatal pathway connects the substantia nigra pars compacta with the basal ganglia, including the dorsal striatum (caudate nucleus and putamen). It is further influenced by the frontal lobes (involved in executive function, problem-solving and controlling behavior).
Mesocortical Pathway– Projections from the ventral tegmental area to the prefrontal cortex. Responsible for behavioral/executive function. The mesocortical pathway uses dopamine to help direct our memory, focus, and decision-making.
Mesolimbic Pathway– Projections from the ventral tegmental area to the forebrain (especially the nucleus accumbens in the basal forebrain). Responsible for emotional function. The mesolimbic pathway is associated with dopamine’s function related to reward and pleasure.
Retinal Fibers– Intrinsic dopaminergic neurons have been identified in the retinas. Patients with Parkinson’s complain of impaired visual function and difficulty reading. Dopamine controls absolute sensitivity, spatial contrast sensitivity, temporal sensitivity, and color vision.
Tuberoinfundibular Pathway– Projections from the hypothalamus to the pituitary gland. The origins of the pathway are classically assigned to the periventricular and arcuate (infundibular) nuclei. The tuberoinfundibular pathway uses dopamine to inhibit prolactin release in the pituitary system, which can stimulate breast milk production.
“Resilience is very different than being numb. Resilience means you experience, you feel, you fail, you hurt. You fall. But, you keep going.” Yasmin Mogahed
Parkinson’s Is Not Just a Dopamine-dependent Motor-deficient Disorder: Because it’s Parkinson’s, it is not easy to understand the wickedness. So to finish up this meandering post, here is a condensed view of other neurotransmitters with dopamine, focusing on some new links to motor defects and the always troublesome non-motor symptoms.
Dopamine– As Parkinson’s progresses, the mesocortical and mesolimbic pathways can become dysfunctional. The loss of dopamine to these dopaminergic systems would contribute to anxiety, depression, apathy, or possibly impulse control disorders.
Serotonin– In concert with dopaminergic neurons dying in Parkinson’s, there is a growing understanding that serotonergic neurons ae also being affected. Reducing serotonin can be implicated in tremors and dyskinesia issues but also includes cognitive problems, depression, fatigue, and hallucinations.
Acetylcholine– Degeneration of cholinergic neurons is found in Alzheimer’s and Parkinson’s. These cholinergic neurons are in the cerebral cortex, seeming there early in the disorder, and when it worsens, dementia may be present. Suppose cholinergic neurons are dying in the brainstem pedunculopontine nucleus. In that case, it may partly explain dopamine non-responsive gait and balance issues with falls.
Norepinephrine– The release of norepinephrine from the locus coeruleus significantly impacts blood pressure and heart rate. The loss of noradrenergic neurons seems to mimic the loss of dopaminergic neurons in Parkinson’s. Since many people with Parkinson’s have orthostatic hypotension, is this related to changes in norepinephrine or dopamine, or both? Deficiency of norepinephrine has also been associated with a postural instability-gait disorder and non-motor features related to apathy, depression, attention impairment, and sleep disturbance.
“Strong lives are those that are marked by a sense of purpose, connectedness, resilience, and fulfillment.” Jenifer Fox
One + One + One +One = Four: You can begin to appreciate why this story is but the tip of the iceberg, right? There is much left to understand, read about, and ponder to unify this story. These neurotransmitter systems are vital to our everyday health. Therefore, it makes sense that if they are becoming dysfunctional as Parkinson’s progresses, they might contribute some of the morbidity to the whole story of Parkinson’s.
I include a final Table, which tries to unify the non-motor symptoms of Parkinson’s with the dysfunctional neurotransmitter system(s) described here. There are some inconsistencies here and in the text (primarily due to the primary source of information). What this tells me is that Parkinson’s is a heterogeneous disorder that alters many structures in the brain as it percolates through various regions to inflict its damage. Awareness of these possible multi-systematic neurotransmitter changes in Parkinson’s opens up a new drawer of pharmacological intervention that may help us down the road as the disorder progresses.
“Resilience is accepting your new reality, even if it’s less good than the one you had before.” Elizabeth Edwards
Conclusions: Stay involved in your disorder. Make sure you tell your healthcare team about the issues behind your Parkinson’s. If some of your symptoms have become non-responsive to dopaminergic therapy and manipulation, it is imperative. I will undoubtedly write more about the interplay of these neurotransmitter systems in Parkinson’s as I gain a better understanding.
To close, remain hopeful about Parkinson’s advances and understanding. The more we learn and peel off another layer of the onion, the closer we are to finding novel and innovative treatment paths for Parkinson’s. Moreover, this new proficiency may lead us to rescue, recover, and heal the brain from our captor, the sinister Parkinson’s.
“There is something in these moments of crisis that is really extraordinary about humanity and human beings’ resilience and the way in which everyone naturally comes together. I think you see the best in people in those moments for better or for worse and you find your best self.” Carla Gugino
Selected References:
Elkouzi, Ahmad, Vinata Vedam-Mai, Robert S. Eisinger, and Michael S. Okun. “Emerging therapies in Parkinson disease—repurposed drugs and new approaches.” Nature Reviews Neurology 15, no. 4 (2019): 204-223.
Mao, Qi, Wang-zhi Qin, Ao Zhang, and Na Ye. “Recent advances in dopaminergic strategies for the treatment of Parkinson’s disease.” Acta Pharmacologica Sinica 41, no. 4 (2020): 471-482.
Charvin, Delphine, Rossella Medori, Robert A. Hauser, and Olivier Rascol. “Therapeutic strategies for Parkinson disease: beyond dopaminergic drugs.” Nature Reviews Drug Discovery 17, no. 11 (2018): 804-822.
Armstrong, Melissa J., and Michael S. Okun. “Diagnosis and treatment of Parkinson disease: a review.” Jama 323, no. 6 (2020): 548-560.
Schapira, Anthony HV, K. Chaudhuri, and Peter Jenner. “Non-motor features of Parkinson disease.” Nature Reviews Neuroscience 18, no. 7 (2017): 435-450.
Marras, Connie, and K. Ray Chaudhuri. “Nonmotor features of Parkinson’s disease subtypes.” Movement Disorders 31, no. 8 (2016): 1095-1102.
Morris, Rosie, Douglas N. Martini, Tara Madhyastha, Valerie E. Kelly, Thomas J. Grabowski, John Nutt, and Fay Horak. “Overview of the cholinergic contribution to gait, balance and falls in Parkinson’s disease.” Parkinsonism & related disorders 63 (2019): 20-30.
Factor, S. A., W. M. McDonald, and F. C. Goldstein. “The role of neurotransmitters in the development of Parkinson’s disease‐related psychosis.” European Journal of Neurology 24, no. 10 (2017): 1244-1254.
Espay, Alberto J., Peter A. LeWitt, and Horacio Kaufmann. “Norepinephrine deficiency in Parkinson’s disease: the case for noradrenergic enhancement.” Movement Disorders 29, no. 14 (2014): 1710-1719.
Delaville, Claire, Philippe De Deurwaerdère, and Abdelhamid Benazzouz. “Noradrenaline and Parkinson’s disease.” Frontiers in systems neuroscience 5 (2011): 31.
Bohnen, Nicolaas I., and Roger L. Albin. “The cholinergic system and Parkinson disease.” Behavioural brain research 221, no. 2 (2011): 564-573.
Maillet, Audrey, Paul Krack, Eugénie Lhommée, Elise Météreau, Hélène Klinger, Emilie Favre, Didier Le Bars et al. “The prominent role of serotonergic degeneration in apathy, anxiety and depression in de novo Parkinson’s disease.” Brain 139, no. 9 (2016): 2486-2502.
Rizzi, Giorgio, and Kelly R. Tan. “Dopamine and acetylcholine, a circuit point of view in Parkinson’s disease.” Frontiers in neural circuits 11 (2017): 110.
Cover photo image by Jonny Belvedere from Pixabay

WOW! Interesting post, Frank. I keep learning, and the more I learn the more I realize that I need to learn…. Describing the interplay of dopamine with the other neurotransmitters represents a brand new layer of the onion for me!
Many thanks for this.
Bill
LikeLike
Thanks, Bill. The topic intrigued me because I had never heard of other neurotransmitters being altered in Parkinson’s. I guess Parkinson’s is clearly not a 1 neurotransmitter-linked disorder. It does complicate the story, and in my mind, it was already reasonably complicated! Happy Holidays! Frank
LikeLike
Thank you. Dr Okun in Florida (Muhammad Ali’s doctor) says PD is the most complex disease of all.
LikeLike
Joe, I would believe such a statement! Frank
LikeLike