


“There is a time for many words, and there is also a time for sleep.” Homer
“Sleep is a hint of lovely oblivion.” D. H. Lawrence
The Problem of Sleep: If you have Parkinson’s, you likely have some problem with sleep. If you have Parkinson’s and you do not have a sleeping problem, then count your blessings. Here is a brief overview of sleeping disorders found in Parkinson’s, some personal issues that I have had with sleeping (and the lack thereof), and the results of a recent personal change in my sleep pattern (let’s call it my “sleep experiment”).
“Early to bed and early to rise makes a man healthy, wealthy and wise.” Benjamin Franklin
The Importance of Sleep: You probably already know all of these reasons, but they are worth revisiting and thinking about how our disrupted sleep pattern in Parkinson’s is affecting our life in the short- and long-term.
I do not know about you, but after a day of life in the presence of Parkinson’s, my mind is exhausted, ready for a shut-down period, and in need of a reviving and replenishing sleep. What benefits does sleep offer anyone with or without Parkinson’s?
•Restoration– I have used this analogy before, think of your brain as a sponge, and as the day progresses, the sponge is filling up with water. During several hours of sleep, the sponge is squeezed, excess fluid and toxic waste are removed, and the function of the sponge (i.e., the brain) is regenerated.
•Resurgence- The CDC suggests that getting an adequate amount of sleep (7–9 hours for adults) is critical for overall good health. Sleep supports physical repair, brain function, and emotional stability. Specifically, the primary benefits of sleep include immune system renewal, enhanced memory and focus, better weight management, reduced stress, and a lower risk of chronic disorders such as heart disease.
The Amount of Sleep Needed as Recommended by the CDC
(U.S. Centers for Disease Control and Prevention)
| Age Group | Age (years) | Hr Sleep Proposed by CDC |
| Adult | 18-59 | 7 or more hours |
| Adult | 60-64 | 7-9 hours |
| Adult | 65 and older | 7-8 hours |
“Sleep is a hint of lovely oblivion.” D. H. Lawrence
OK, what happens if we don’t get 7-9 hours of sleep each night? It means we are chronically sleep-deprived, and over time, we may become susceptible to disruptions in our routine health. I am not questioning that we need more sleep, and I am not disclaiming the health benefits of adequate sleep; I just wish getting more sleep in the presence of Parkinson’s would be easy to accomplish. I really think that a continued lack of sleep clearly favors Parkinson’s gaining leverage on our brains and creating an environment that favors the progression of Parkinson’s.
“Sleep is like the unicorn – it is rumored to exist, but I doubt I will see any” Dr. Seuss
Sleep Disorders in Parkinson’s: Part of the problem is made more difficult when one considers that Parkinson’s has a wide array of sleep disorders in individuals with Parkinson’s. Like everything else in Parkinson’s, a “one-size-fits-all” approach does not work for everyone. Below is a list of the most common sleep disorders found in Parkinson’s; however, I will not go further into their description:
The Most Common Sleep Disorders in Parkinson’s Disease (PD)
Circadian dysfunction
Excessive daytime sleepiness
Insomnia
Obstructive sleep apnea in PD
REM Sleep Behavior Disorder (RBD)
Restless leg syndrome in PD
“Sleep is the most blessed and blessing of all natural graces.” Aldous Huxley
My Sleeping Problems: I have never slept the recommended hours as suggested above, either with or without Parkinson’s. However, the past several years have led me to study sleep issues in Parkinson’s, to read several reviews about sleep issues in Parkinson’s, and to write about sleep issues in Parkinson’s. This much I have learned: first, my Parkinson’s symptoms are helped by getting “quality” sleep. And second, my Parkinson’s medications work better when I have had “quality” sleep. I realize I need to get “more” hours of sleep, but I keep coming back to the idea that, for me, the quality of my sleep is sometimes better than the quantity. It just seems to me that my Parkinson’s does not like it when I get a quality 5-6 hours of sleep compared to an up-and-down but of lesser quality 7-8 hours of sleep.
My sleep problem is not falling asleep; it is staying asleep. This is confounded by occasional vivid dreams and the even less frequent RBD-linked nightmares. Like many individuals with Parkinson’s, I also have obstructive sleep apnea (OSA), and I use a CPAP (or Continuous Positive Air Pressure) machine to provide an open airway during the night.
“A ruffled mind makes a restless pillow.” Charlotte Bronte
My latest attempt to improve both the quality and quantity of sleep: I had my second total hip replacement surgery in early January, and this time of recovery led me to commit to a new plan to ‘improve’ my sleep. Like everything else presented here, this is the plan I have developed for myself; it has an n=1. I present it with the disclaimer that you should consult your own Neurologist before even considering any of the ideas in this blog post. It is provided for your information and to give you a sense of what I am currently doing to improve my sleep. I do not know if following any of these steps would help you with your sleep issues, but it might give you a framework to begin formulating your own set of instructions.
•First, the notion of clearing out your brain in the evening is something new for me, but it makes sense. I have had so many late nights, all-nighters, writing this blog. I do not even want to go there. Thus, I am making an honest attempt to wind down in the evening, beginning at 9:00-10:00 PM or 21:00-22:00 (using a 24-hour clock), with no reading, thinking about a future blog article, or anything related to Parkinson’s. I use this time to take the evening’s take of supplements slowly, I may still have music playing or the TV on, but I am not ‘focused’ on it. The goal has been to standardize when and how I fall asleep, in the absence of plans for tomorrow and beyond, or of deliberate/conscious thoughts.
•Second, adding several supplements to aid my sleep. If you read this blog, then you know I have tried and used several different types of supplements to enable my battle against Parkinson’s. It is not that I think they are curative, I feel that supplements are either replacing an essential survival ingredient taken away by the disease process, that is, drained or consumed from the physiological process. Furthermore, some supplements have been used in an attempt to quench an environmental disaster created by the disease process. Threfore, by adding vitamins to my daily regimen fulfills the first goal, and by adding antioxidants and anti-inflammatory compounds to quench the fire in the second goal. This gives you my logic for trying supplements targeted to improve my sleep habits.
“Rock ‘n’ roll never sleeps it just passes out.” George Thorogood
Glycine, Magnesium Threonate, Apigenin, and Melatonin: While there are many possible supplements to choose and evaluate for enabling sleep, I have chosen these specifically. The structures of Glycine, Magnesium Threonate, Apigenin, and Melatonin are illustrated below.
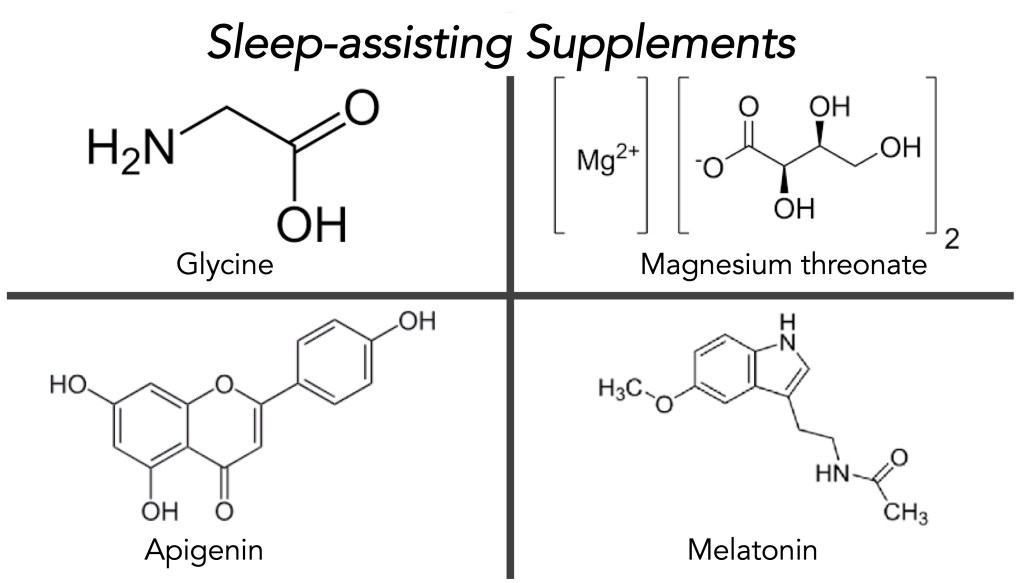
•Glycine– Glycine is an amino acid, the simplest of the 20 natural amino acids. Glycine can cross the blood-brain barrier and acts as an inhibitory neurotransmitter. In sleep-assisting, glycine has been found to improve sleep quality by lowering core body temperature, stabilizing the sleep process, and increasing deep sleep. Apparently, glycine acts on NMDA receptors, producing a calming effect, and induces vasodilation to help the body lose heat, all in all signaling to the brain that it is time to sleep. Importantly, glycine does not create a morning hangover or grogginess. The majority of sleep studies use 3 grams of glycine, taken approximately 30-60 minutes before bedtime. Please note that I have taken either 500 mg or 1000 mg at the most in my use of glycine. If you try glycine for sleeping, I would start with 500 mg and work your way up over a few weeks, and slowly increase the dose. The current source of glycine I am using is from Double Woods Supplements, each has 500 mg of glycine (click here).
•Magnesium threonate– Magnesium threonate (branded name of Magtein) is the most bioavailable form of magnesium to enter the brain. Magtein crosses the blood-brain barrier and has been found to improve sleep quality, enhancing deep sleep and REM sleep. Evidently, magnesium helps regulate neurotransmitters and the circadian rhythm, thereby improving sleep quality. Most studies have used 145-200 mg of elemental magnesium. The typical daily dose of Magtein is 3-4 capsules [2 in the morning and 2 in the evening (this translates to 2000 mg Magtein and 144 mg elemental magnesium per day)]. Please note that in past studies, taking 3-4 capsules of Magtein daily led to daytime sleepiness. For its current use, I take a single Magtein capsule 30-60 minutes before bedtime. The Magtein source I am currently using is Double Woods Supplements. Taking one capsule provides 500 mg of Magtein and 36 mg of elemental magnesium (click here).
•Apigenin– Apigenin is a flavonoid and acts as a mild sedative that promotes relaxation to improve sleep quality. Apigenin binds to GABA receptors and, as a supplement, has been used at 50-300 mg 30-60 minutes before bedtime. The clinical evidence suggests that apigenin, when derived from its natural source, chamomile, does promote improved sleep, but the use of purified supplements is limited. Please note that due to its sedative properties, I have never used more than 50 mg in my own studies. The source of apigenin I am currently taking is Double Supplements Woods, in 50 mg capsules (click here).
•Melatonin– Likely, when you mentioned you were having problems sleeping, your Neurologist suggested trying melatonin. They might have suggested you try 5-10 mg of melatonin 30-60 minutes before bedtime. Moreover, if that did not work, some patients increased their melatonin to 15 mg nightly. When I tried 5 mg of melatonin, I was barely able to stay awake the next day; it just hit me like a brick. We produce melatonin in our pineal gland. Melatonin regulates the sleep-wake cycle and has been widely used as a short-term supplement to help with jet lag, day-night work shifts, and to reduce the time to fall asleep. It is thought to be a safe product, but only when used in the short term; few studies have been done long term (i.e., longer than a few weeks). Part of the difficulty with melatonin is the wide discrepancy in the actual amount of melatonin across products (it is not a regulated product, and quality issues have been noted).
I began studying the sources of melatonin and the amounts available. We produce about 300 micrograms (0.3 milligrams) of melatonin per day. Thus, I found two products that sold melatonin in 300 microgram capsules: the first was Life Extension Melatonin (300 mcg or 300 micrograms) (click here), and the second was Carlyle Melatonin (300 mcg or 300 micrograms) (click here). Clearly, I have some issues with processing melatonin, and I am very sensitive to amounts of the supplement that are routinely used by many individuals with Parkinson’s. Please note that I take 1 or 2 capsules of melatonin (about 300-600 micrograms) 30-60 minutes before bedtime.
Based on many suggestions, I would carefully evaluate your use of melatonin and possibly only use it for a few weeks, then stop for a few weeks before returning to it. As discussed by many reputable medical schools/hospitals, melatonin should be used carefully, only after speaking with your Neurologist.
“The best eraser in the world is a good night’s sleep.” Orlando Aloysius Battista
•Nap Time- I must add that included in this ‘experiment’ was the event of taking naps in the afternoon. Over the past year, I have increased the time I spend napping. Maybe this is a luxury, maybe it is part of the disease process, but naps usually give me renewed, positive feelings. My reason for taking naps is partly based on the dopaminergic therapy we typically take, which frequently comes with increased daytime sleepiness, as well as part of the disorder. My philosophy on napping is based on how my body feels when I ‘need’ one. It feels like a necessity. Furthermore, a nap can last from 20-90 minutes. Please note that my nap-taking time and frequency have not increased or changed since adding these supplements.
“A well-spent day brings happy sleep.” Leonardo da Vinci
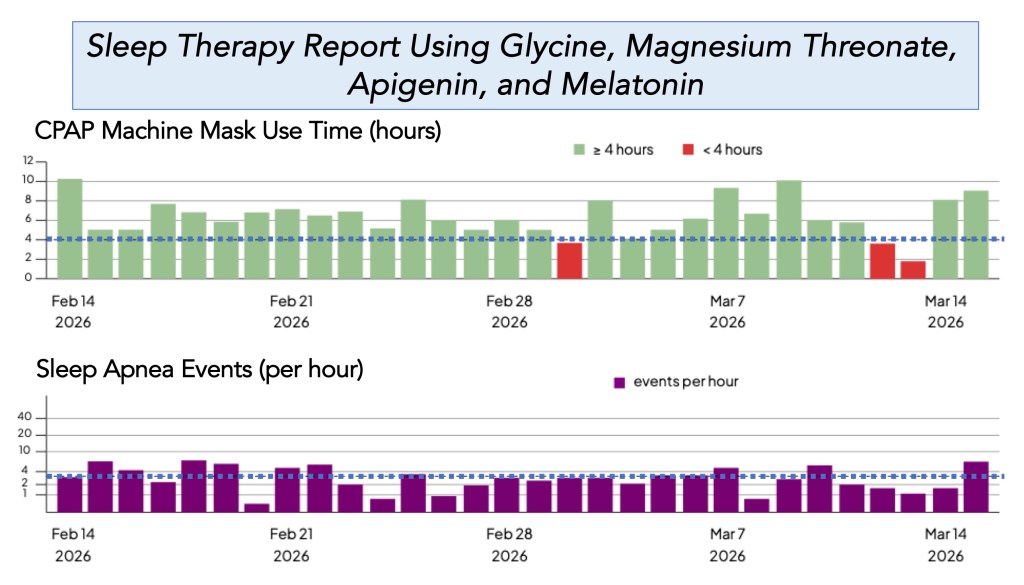
•Results in Progress– I have been using the above schedule of supplements since January 2026 (actually, after my hip replacement surgery on 01/12/2026). As described by Patel et al. (Patel AK, Reddy V, Shumway KR, et al. Physiology, Sleep Stages. [Updated 2024 Jan 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526132/), humans cycle through 2 phases of sleep, (1) rapid eye movement (REM) and (2) nonrapid eye movement (NREM) sleep, which is further divided into 3 stages—N1 to N3. The body cycles through all stages approximately 4 to 6 times each night, with each cycle averaging 90 minutes. As many use data from their iWatch to plot these amounts for various sleep cycle components, I am initially interested in how much time I spend wearing my CPAP mask and using the machine. Why? Because I am first interested in understanding whether I can sleep longer each night with these supplements, and this is a regular, reliable process for me to use.
Before starting this ‘deliberate attempt’ to improve my sleep habits, I was averaging about 3-4 hours of CPAP machine time. As shown below, over the past 30 days, my average CPAP machine mask time was 6 hours 22 minutes (top plot). The data below show that I had 27 of 30 days (90%) in which I achieved greater than 4 hours of sleep using the CPAP machine, and 18 of 30 days of greater than or equal to 6 hours. The two recent dates of <4 were an out-of-town trip to Ponte Vedra, Florida, to watch some of the Players Golf Championship (I do not sleep well the first few days in a new environment). Shown below the mask time is the number of sleep apnea events I had each evening. Thus, the number of events is met when the value is <4 events per hour per day (without the CPAP machine, my sleep study revealed that I could have 25-35 apnea events/hr/night).
“I love sleep. My life has the tendency to fall apart when I’m awake, you know?” Ernest Hemingway
Typical Format of a Day-Night: The day was filled with trips to the post office and grocery store. I am still rehabilitating my new left hip, so I do a lot of stretching exercises daily. We finished dinner about 8:15 PM. I began my evening slowdown around 9:45 PM. Took the following supplements: one capsule of 0.3 mg melatonin, two capsules of 500 mg glycine, one capsule of 500 mg magnesium threonate (36 mg elemental magnesium), and one capsule of 50 mg of apigenin. I then took my fourth anti-Parkinson’s treatment with Crexont (1 capsule of 350 mg levodopa/87.5 mg carbidopa, and 1 capsule of 280 mg levodopa/70 mg carbidopa). Put on a CPAP mask and started the CPAP machine at 11:00 PM. Total CPAP mask/machine time was 7 hr 38 min, with 2.7 breathing events per hour (a score of <4 is really good), and woke up needing a bathroom break at ~4:00 AM. Fell back to sleep in ~5 min. Woke up feeling refreshed and was not groggy, felt well-rested, and got ready for a physical therapy appointment at 9:00 AM.
“A night of sleep is as much preparation for the subsequent day’s activity as it is recovery from that of the previous day.” J. Allan Hobson
Summary: This blog post aimed to improve my sleep habits. I started by changing the nightly pattern of approaching sleep (including the little things like stopping caffeinated beverages by mid to late afternoon). And then I added and evaluated four supplements.
Try glycine and magnesium threonate first, either individually or together. Obviously, start with small amounts (1 capsule of 500 mg glycine and 1 capsule of Magtein) for a few weeks, and see if your sleep quality and amount improve. Then try apigenin (1 capsule of 50 mg). Melatonin should be tested for your individual sensitivity, starting with a 1 mg dose for a week, then increasing by 1 mg increments until you find the dose that best promotes sleep without a residual grogginess. Others like me are sensitive to melatonin and its impact to cause drowsiness the next day at very low doses.
Medical Disclaimer:
This blog post contains information related to health care. It is not intended to replace medical advice. It should be used to supplement, rather than replace, your neurologist’s regular care. It is recommended that you seek your physician’s advice/approval before embarking on any new health plan or changes to your existing plan/routine.
Please note that the views and opinions expressed here are my own. I am not a physician, and this content is presented for informational purposes only and not as medical advice. Just because I take these supplements does not prove their safety and efficacy. Please consult your neurologist/physician if you are interested in this material.
“I had a new idea in my head… this time it’s just simply my bedroom, only here colour is to do everything, and, giving by its simplification a grander style to things, is to be suggestive here of rest or of sleep in general. In a word, to look at the picture ought to rest the brain or rather the imagination.” Vincent Van Gogh
References
Parkinson’s and Sleep Disorders-
Loddo, Giuseppe, Giovanna Calandra-Buonaura, Luisa Sambati, Giulia Giannini, Annagrazia Cecere, Pietro Cortelli, and Federica Provini. “The treatment of sleep disorders in Parkinson’s disease: from research to clinical practice.” Frontiers in neurology 8 (2017): 42.
Stocchi, Fabrizio, Luca Barbato, Giampietro Nordera, Alfredo Berardelli, and Stefano Ruggieri. “Sleep disorders in Parkinson’s disease.” Journal of Neurology 245, no. Suppl 1 (1998): S15-S18.
Larsen, Jan P., and Elise Tandberg. “Sleep disorders in patients with Parkinson’s disease: epidemiology and management.” CNS drugs 15, no. 4 (2001): 267-275.
Taximaimaiti, Reyisha, Xingguang Luo, and Xiao-Ping Wang. “Pharmacological and non-pharmacological treatments of sleep disorders in Parkinson’s disease.” Current neuropharmacology 19, no. 12 (2021): 2233-2249.
Glycine-
Bannai, Makoto, and Nobuhiro Kawai. “New therapeutic strategy for amino acid medicine: glycine improves the quality of sleep.” Journal of pharmacological sciences 118, no. 2 (2012): 145-148.
Yamadera, Wataru, Kentaro Inagawa, Shintaro Chiba, Makoto Bannai, Michio Takahashi, and Kazuhiko Nakayama. “Glycine ingestion improves subjective sleep quality in human volunteers, correlating with polysomnographic changes.” Sleep and Biological Rhythms 5, no. 2 (2007): 126-131.
Kawai, Nobuhiro, Noriaki Sakai, Masashi Okuro, Sachie Karakawa, Yosuke Tsuneyoshi, Noriko Kawasaki, Tomoko Takeda, Makoto Bannai, and Seiji Nishino. “The sleep-promoting and hypothermic effects of glycine are mediated by NMDA receptors in the suprachiasmatic nucleus.” Neuropsychopharmacology 40, no. 6 (2015): 1405-1416.
Magnesium Threonate-
Hausenblas, Heather A., Tarah Lynch, Stephanie Hooper, Aahana Shrestha, Doug Rosendale, and Jennifer Gu. “Magnesium-L-threonate improves sleep quality and daytime functioning in adults with self-reported sleep problems: A randomized controlled trial.” Sleep medicine: X 8 (2024): 100121.
Lopresti, Adrian L., and Stephen J. Smith. “The effects of magnesium L-threonate (Magtein®) on cognitive performance and sleep quality in adults: a randomised, double-blind, placebo-controlled trial.” Frontiers in Nutrition 12 (2025): 1729164.
Arab, Arman, Nahid Rafie, Reza Amani, and Fatemeh Shirani. “The role of magnesium in sleep health: a systematic review of available literature.” Biological trace element research 201, no. 1 (2023): 121-128.
Chan, Vicky, and Kenneth Lo. “Efficacy of dietary supplements on improving sleep quality: a systematic review and meta-analysis.” Postgraduate medical journal 98, no. 1158 (2022): 285-293.
Apigenin–
Kramer, Daniel J., and Adiv A. Johnson. “Apigenin: a natural molecule at the intersection of sleep and aging.” Frontiers in Nutrition 11 (2024): 1359176.
Wong, Wing-Yan, Brandon Dow Chan, Hengshen Zhou, Tsz Chun Leung, and William Chi-Shing Tai. “Synergistic sleep-promoting effects of magnesium and apigenin in normal and insomnia mouse models.” Food & Function (2026).
Salehi, Bahare, Alessandro Venditti, Mehdi Sharifi-Rad, Dorota Kręgiel, Javad Sharifi-Rad, Alessandra Durazzo, Massimo Lucarini et al. “The therapeutic potential of apigenin.” International journal of molecular sciences 20, no. 6 (2019): 1305.
Mushtaq, Zarina, Nabeelah Bibi Sadeer, Muzzamal Hussain, Mahwish, Suliman A. Alsagaby, Muhammad Imran, Tamseela Mumtaz et al. “Therapeutical properties of apigenin: a review on the experimental evidence and basic mechanisms.” International Journal of Food Properties 26, no. 1 (2023): 1914-1939.
Melatonin-
Fatemeh, Gholami, Moradi Sajjad, Rasaei Niloufar, Soveid Neda, Setayesh Leila, and Mirzaei Khadijeh. “Effect of melatonin supplementation on sleep quality: a systematic review and meta-analysis of randomized controlled trials.” Journal of neurology 269, no. 1 (2022): 205-216.
Poza, Juan Jose, Montserrat Pujol, Juan Jose Ortega-Albás, and O. Romero. “Melatonin in sleep disorders.” Neurología (English Edition) 37, no. 7 (2022): 575-585.
Ferracioli-Oda, Eduardo, Ahmad Qawasmi, and Michael H. Bloch. “Meta-analysis: melatonin for the treatment of primary sleep disorders.” PloS one 8, no. 5 (2013): e63773.
Grigg-Damberger, Madeleine M., and Dessislava Ianakieva. “Poor quality control of over-the-counter melatonin: what they say is often not what you get.” Journal of Clinical Sleep Medicine 13, no. 2 (2017): 163-165.
Cover Photo Image by Greg Montani from Pixabay
