


“Don’t wish it were easier, wish you were better.” Jim Rohn
“Mostly everything gets worse before it gets better.” Wanda Sykes
Introduction: A neurodegenerative disease occurs when neurons in the brain begin to lose their function and ultimately die. The two most important and prevalent neurodegenerative disorders are Alzheimer’s and Parkinson’s. One of my earliest and most widely read blog posts is “A Comparison of Parkinson’s to Alzheimer’s” (click here to read this post). A common issue with both disorders is the accumulation of neurotoxic proteins that, with time, perturb, damage, and eventually result in neuronal cells dying. However, the expression of these disorders occurs in different parts of the brain.
Furthermore, the neurotoxic proteins are different in Alzheimer’s compared to Parkinson’s. And you are likely already aware that typically Parkinson’s is more dominant in motor dysfunction, followed by other defects. While Alzheimer’s usually begins as a cognitive defect, followed by additional anomalies. I have always believed, maybe naively, that any success in halting the deposition of toxic protein components in one disorder could potentially be applied and tested in the other disorder.
The effectiveness of a novel substance, Buntanetap, is presented by Fang and associates, in the treatment of Parkinson’s and Alzheimer’s [Fang, Cheng, P. Hernandez, K. Liow, E. Damiano, Henrik Zetterberg, Kaj Blennow, D. Feng, M. Chen, and M. Maccecchini. “Buntanetap, a Novel Translational Inhibitor of Multiple Neurotoxic Proteins, Proves to Be Safe and Promising in Both Alzheimer’s and Parkinson’s Patients.” The Journal of Prevention of Alzheimer’s Disease 10, no. 1 (2023): 25-33]. This is a detailed paper with interesting clinical observations using buntanetap to treat patients with Alzheimer’s or Parkinson’s.
“People say it gets better but it doesn’t. It just gets different, that’s all.” Maggie Smith
Background Science Lesson: The Central Dogma of Life explains how we follow instructions to convert DNA into a final product. The flow of the central dogma follows that DNA is replicated. Then DNA is converted to small segments of RNA in a process called transcription. Finally, following essential instructions, RNA, in translation, encodes for a growing polypeptide chain that assembles into a protein. Converting DNA into a protein is more commonly called gene expression.
It is more complicated than this with the discovery of reverse transcriptase that converts RNA to DNA (an example would be the retroviruses, i.e., HIV) and the evolving role of small RNA molecules in molecular biology, but this is way beyond the intention of this introduction. The drawing below summarizes the central dogma.

“Your life does not get better by chance, it gets better by change.” Jim Rohn
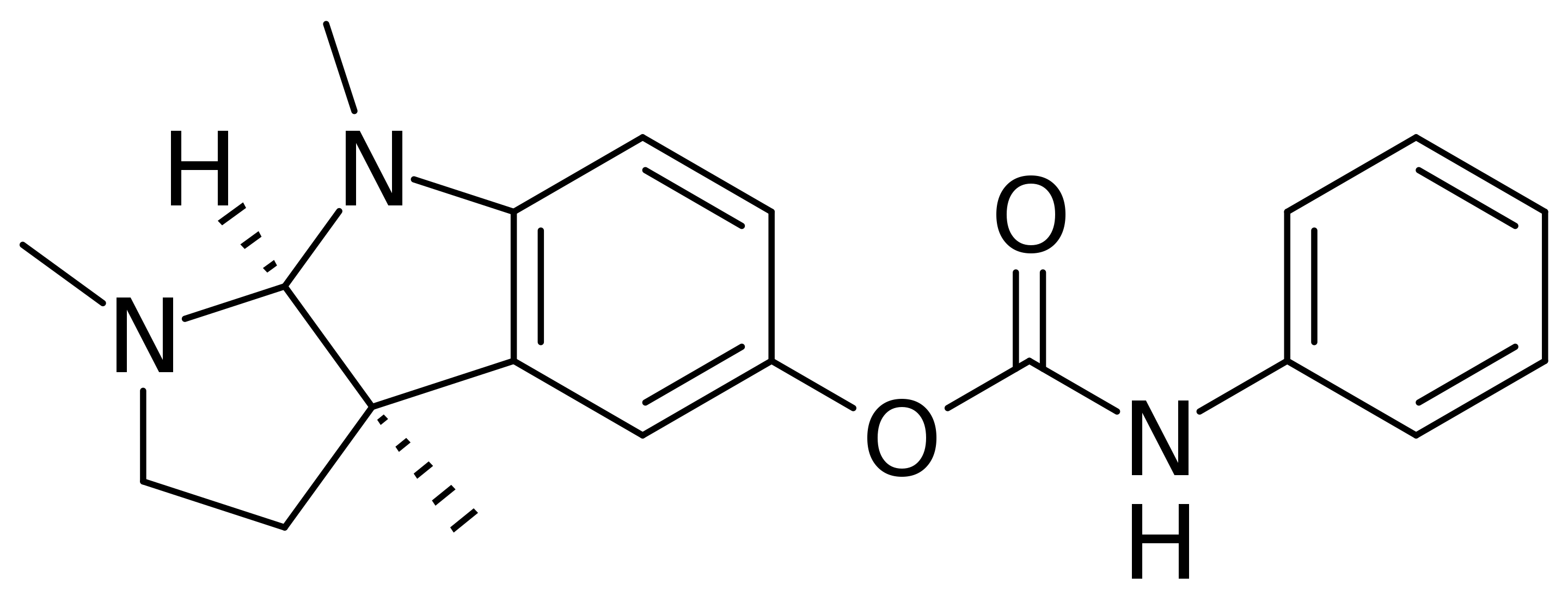
Buntanetap is a Translation Inhibitor: Buntanetap (also known as ANVS401 or Posiphen) is an orally bioavailable molecule first discovered by the National Institutes of Aging in Bethesda, MD. The structure of Buntanetap is shown below:
Buntanetap suppresses the translation of mRNAs of neurotoxic aggregating proteins in Parkinson’s and Alzheimer’s disease. Specifically, these neurotoxic proteins are alpha-synuclein (aSYN), a hallmark pathogenic product in Parkinson’s. Furthermore, amyloid precursor protein (APP), β-amyloid (Aβ), and tau neurofibrillary tangles are the pathogenic protein participants in Alzheimer’s.
Buntanetap works by suppressing the translation of the mRNA’s of aSYN, APP, and tau by enhancing the binding of the atypical response element (IRE) in these neurotoxic proteins’ mRNAs 5’UTR (untranslated region) to iron regulatory protein 1 (IRP1) in the presence of high iron. The ability of buntanetap to specifically prevent the translation of these neurotoxic substances is essentially ‘molecular magic.’ It makes my brain hurt thinking about the process. Amazing.
“In my opinion, the only way to conquer stage fright is to get up on stage and play. Every time you play another show, it gets better and better.” ~ Taylor Swift
Working Hypothesis for Buntanetap to Slow Progression of Parkinson’s and Alzheimer’s: Experimentally, buntanetap can block several neurotoxic proteins’ expression. Therefore, the hypothesis being tested is that buntanetap ‘normalizes’ the levels of these toxic proteins in Parkinson’s and Alzheimer’s. Theoretically, this would allow proteostasis to commence, which is the process that regulates proteins within the cell and the organism to maintain health. Additionally, stopping the accumulation of these neurotoxic proteins could rescue neuronal cell function, prevent nerve cell death, and potentially halt further neurodegeneration.
•Animal Models Studies Support the Function of Buntanetap in Neurodegenerative Disorders–
I realize that some readers do not like the existing animal models to begin testing molecules for therapeutic ability. The necessary transition typically goes from synthesis, in vitro testing, cell lines in tissue culture, and then to small animal disease models (usually mice and rats). Many animal models for Parkinson’s and Alzheimer’s have been developed. They offer the investigator a model that can recapitulate certain aspects of these disorders. They are helpful but far from perfect. Data has been published in several animal models to advance the working hypothesis of buntanetap. Dr. Maria Maccecchini gave this presentation at an International Alzheimer’s Conference entitled “P3-852 – Do Mouse Data Lie? For Buntanetap, They Totally Predict Human Outcome” (click here to read).
•Inital Clinical Evaluation of Buntanetap–
Buntanetap was first evaluated in five patients with mild cognitive impairment. The drug was generally safe and well-tolerated. After treatment for 10 days with buntanetap, the patients had reduced APP levels, total tau, and a-SYN. These results supported the hypothesis that buntanetap could reduce the levels of neurotoxic proteins in neurodegenerative disorders. For further information, see this paper: Maccecchini, Maria L., Mee Young Chang, Catherine Pan, Varghese John, Henrik Zetterberg, and Nigel H. Greig. “Posiphen as a candidate drug to lower CSF amyloid precursor protein, amyloid-β peptide and τ levels: target engagement, tolerability and pharmacokinetics in humans.” Journal of Neurology, Neurosurgery & Psychiatry 83, no. 9 (2012): 894-902.
“One doesn’t discover new lands without consenting to lose sight, for a very long time, of the shore.” Andre Gide
The Current Clinical Trial With Buntanetap: There were certain guideposts to achieve, and this included: a larger patient population, the use of a more extended dosing period, and the enrollment of both Alzheimer’s and Parkinson’s patients into the study.
•Study Design- Double-blind, placebo-controlled, and multi-center.
•Patients Studied- 14 early Alzheimer’s and 54 early Parkinson’s patients.
•Drug Amount Used- Alzheimer’s patients were given 80 mg of buntanetap or a placebo. Parkinson’s patients were given 5, 10, 20, 40, or 80 mg buntanetap or placebo.
•Buntanetap was safe and well-tolerated by Alzheimer’s and Parkinson’s patients– A half-time was determined for buntanetap. It was 4-5 hrs.
•Buntanetap improved cognition in Alzheimer’s- Cognition was evaluated using ADAS-Cog11 and WAIS-coding tests. The buntanetap treatment group statistically improved 4.40+2.04 points, while the placebo improved slightly at 1.1 +2.63 points. WAIS-coding measures visual-motor dexterity, associative nonverbal learning, and non-verbal short-term memory. Buntanetap-treated Alzheimer’s patients gave a 6.6+3.04 points improvement, which provided a statistically improved score over placebo samples.
•Buntanetap improved mobility in Parkinson’s– Using Part III of the MDS-UPDRS to measure motor function, they found that buntanetap improved a patient’s mobility. The best improvement was found with 10mg (statistically significant) and 20 mg buntanetap (See Figure below).

•Buntanetap reduced neurotoxic proteins and inflammation in both Alzheimer’s and Parkinson’s patients– Biomarkers for neurotoxic proteins were reduced by Buntanetap in the Alzheimer’s patients, showing a trend for reduction (they argue that the sample size was not sufficient to see a statistical significance). The highest amount of buntanetap (80 mg) reduced Aβ40, sAPPα, sAPPβ, t-tau, and p-tau, the most critical neurotoxic proteins in Alzheimer’s. These results are shown below in the Figure, panel A. Interestingly, they also examined several inflammatory markers and found that those measured were reduced, implying that as the neurotoxic substances were reduced, inflammation was quenched.

The 14 Parkinson’s patients given 80 mg of buntanetap had reduced levels of a-SYN, and they argue that statistical significance was not reached due to sample size (Panel D, Figure above). Significantly, as with Alzheimer’s, the inflammatory markers measured were reduced in those treated with buntanetap in the Parkinson’s patients (again, 80 mg compared to placebo).
•Buntanetap improved neuronal function in Alzheimer’s and Parkinson’s– The two biomarkers examined were neurofilament light (NFL) and neurogranin (NG). NFL is thought to be a marker of neuroaxonal damage, while NG is involved in the regeneration of synapses. In both settings, the changes in characteristics indicate that buntanetap possibly reduces the damage to neuronal cells in both Alzheimer’s (panel C) and Parkinson’s (panel F), see Figure below.

•Discussion– There are some promising findings here. First, buntanetap is well tolerated up to 80 mg. Although not statistically significant, the trend for biomarkers is in the right direction. Their results suggest that buntanetap can reduce levels of neurotoxic proteins, decrease inflammation and improve neuronal cell function. If one believes that neurotoxic proteins contribute to the pathogenic mechanism of these disorders, then the buntanetap results are encouraging. The surprising findings are improved cognition (Alzheimer’s patients) and motor function (Parkinson’s patients) in a treatment scheme of only 25 days. The authors argue that buntanetap might function as a symptomatic drug to relieve neurological symptoms quickly. However, based on their animal studies, they feel that buntanetap is more likely a disease-modifying substance.
“All your dreams can come true if you have the courage to pursue them.” Walt Disney
Conclusions: Parkison’s and Alzheimer’s are complex diseases. The data trend (remember, it was not statistically significant) for buntanetap fits the hypothesis being tested. More encouraging, the directions for reducing neurotoxic proteins, reducing inflammation, and improving neuronal cell function, are somewhat correlated with improved cognition (in Alzheimer’s patients) and motor function (in Parkinson’s patients). The authors are currently planning new clinical trials. It appears that the use of buntanetap is progressing, and the results suggest further testing is warranted.
NOTE ADDED IN PROOF: A few readers have asked about the process for finding out how to apply to a given clinical trial (click her to access website). Furthermore, regarding buntanetap, it has progressed in clinical evaluation by getting through phase 2b and phase 3 trials (additional information can be obtained through the Annovis bio website). Finally, information directly regarding the Phase 3 trial of “Buntanetap for PD” (N=450) can be found here: https://classic.clinicaltrials.gov/ct2/show/NCT05357989.
“Keep believing in brighter days, finding ways for your dreams and wishes to come true. Giving you hope that is as certain as the sun, giving you strength of serenity as your guide.” Douglas Pagels

Excellent article very hopeful.
LikeLike
Thanks, Paulette, I agree it is hopeful. Frank
LikeLike
“The authors are currently planning new clinical trials.”
Also, a Phase 3 trial of “Buntanetap for PD” (N=450) is currently underway.
Estimated Primary Completion Date: December 1, 2023
Estimated Study Completion Date: December 2023
https://classic.clinicaltrials.gov/ct2/show/NCT05357989
LikeLike
Jeff, thanks for this update and information! Frank
LikeLike
Jeff, thanks, I will add an addendum and include this information. Frank
LikeLike
Thank you for your emails…very helpful and interesting…
LikeLike
Interesting and promising information.
How would a person with Parkinson’s look into joining the clinical trial?
Thank you!
LikeLike
Linda,
thanks for the note.
I would go here: Finding a Clinical Trial
Good luck in your journey,
Frank
LikeLike
Let me try this again, go here: Finding a Clinical Trial
https://www.nih.gov/health-information/nih-clinical-research-trials-you
LikeLike
Hello Frank,
I am a person w/ parkinson’s and a past participant in both phase 2b and phase 3 trials for Annovis bio’s buntanetap. I finished the 6 month phase 3 in JUN2023 and am looking to the opportunity to use it during and open label use period for phase 3 participants in early 2024 (post FDA review of phase 3). Your article contained several pieces of information that I wasn’t aware of previously so thank you. For others interested in future tests you can visit the Annovis Bio website.
LikeLike
John, thank you for your note. Always pleased when someone learns something from a blog post. Your experiences with both phase 2b and 3 clinical testing of buntanetap much be both gratifying and hopeful? I have added an ‘addendum’ to the blog post with additional information regarding clinical trials and buntanetap. Thanks so much for writing. Best wishes, Frank
LikeLike