


“The greatest achievement is to outperform yourself.” Denis Waitley
“Sometimes, carrying on, just carrying on, is the superhuman achievement.” Albert Camus
Introduction: Have you been taking carbidopa/levodopa to treat your Parkinson’s? Are you experiencing any off-on periods? Do you have any dyskinesia? Do you think it’s time to change your dosing pattern or the timing of when you take your dose? If the answer is yes to any of these questions, please head to John Turner’s website entitled “Parkinson’s Measurement” (click here to access the site).
This site contains plotting tools and analytical methods to help a person-with-Parkinson’s (PwP). The idea behind this site is to provide these beneficial ‘tools’ for anyone with Parkinson’s and ask you, if willing, to join in their collective research studies. The site is a treasure chest of analytical tools/plotting/programs that can enable PwP to study themselves on various topics. John is to be congratulated on developing such an essential website for Parkinson’s.
For example, below is an analysis of my daily take of levodopa and some changes I am thinking about making based on analytical tools in Parkinson’s Measurement.
*A medical disclaimer is included at the bottom of this post.
“It’s not what you start in life, it’s what you finish.” Katharine Hepburn
Background Information: For the past 18 months, I have been taking generic IR [immediate release carbidopa/levodopa (25/100); and yes, I have a pill cutter, and I take 1/2 tablet on a routine basis] and the Neupro (6 mg Rotigotine dopamine agonist) patch. I take 12 tablets per day and apply one patch per day. The timing of the day is as follows, and it is based on a 4-hour timeframe between treatments:
7 AM, 2.5 tablets = 250 mg levodopa
11 AM, 2.5 tablets = 250 mg levodopa
3 PM, 2.5 tablets = 250 mg levodopa
7 PM, 2.5 tablets = 250 mg levodopa
11 PM, 2 tablets = 200 mg levodopa
Total amount of levodopa/day = 1200 mg.
7:30 AM, Neupro patch (6 mg, a levodopa-equivalence dose = 180 mg levodopa), which gives a levodopa equivalent daily dose (LEDD) = 1380 mg.
“We are made to persist. that’s how we find out who we are.” Tobias Wolff
The Daily Take: Primarily, if I manage my stress levels, I work pretty well throughout the day with this strategy of levodopa and timing. Sometimes in the morning, my right arm tremors are a little whacky, making me wonder about levodopa timing and amount. Sometimes I play early morning golf and take my second dose of levodopa an hour earlier (10 AM instead of 11 AM). I am convinced that dopamine improves your balance, assists in fine motor movements of the golf swing, and it strengthens your stance and entire body.
Suppose something is acting up with the day, stress, overly tired, or just out of sync with the day. In that case, I will take 1/2 tablet and stick it under my tongue to get into the bloodstream faster, and the other two tablets by mouth and swallowing. There are times when I feel I should increase my amounts of levodopa. And are days when I think I should reduce my levodopa dosing scheme.
“Failure I can live with. Not trying is what I can’t handle!” Sanya Richards-Ross
Mapping the Levodopa Day: To measure the levodopa levels during a 24-hour period, I used the John Turner site program entitled “Levodopa Equivalent Minute to Minute Plasma Levels Calculator.”
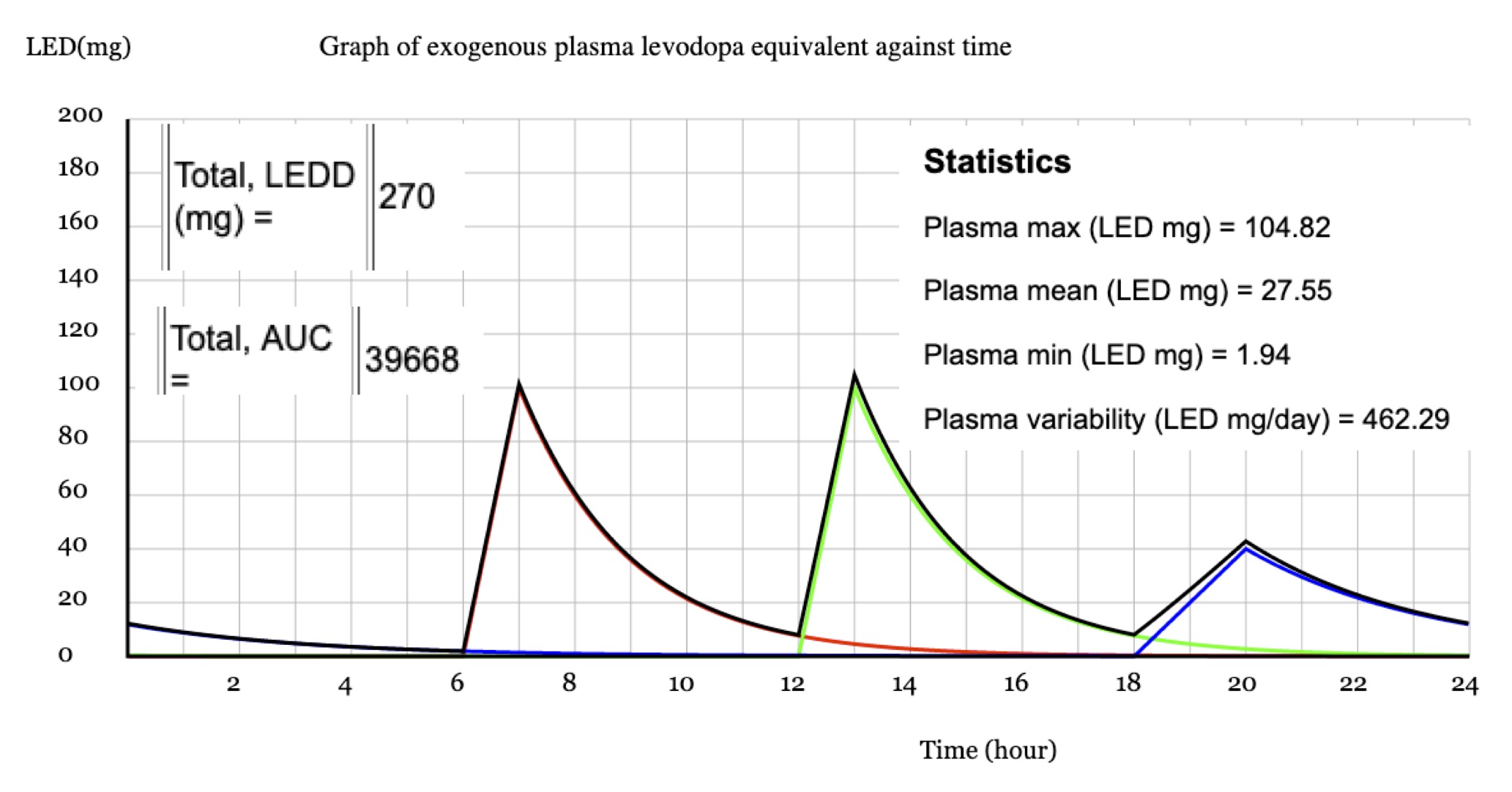
An Example- You will need to enter three things, the time of the dose, the name of the substance being taken, and the amount (in milligrams of levodopa, mg). For instance, you are taking one tablet of the typical size of levodopa (25 mg carbidopa/100 mg levodopa IR) twice per day, and a third time you take levodopa CR times a day, every 6 hours starting at 6:00 AM: you would have three entries in a 24-hour day:
Time (using military timing), Drug Name, and Dose (mg), respectively:
6, Levodopa, 100;
12, Levodopa, 100;
18, Levodopa CR, 100.
Press the “Calculate” button.
You will get the plot below with these amounts based on the levodopa equivalent dose (LED). And it gives you some calculations, such as plasma max, mean, and min (all in LED mg), and it tells you the total levodopa equivalent daily dose or LEDD in mg ). The programmer must make some assumptions in determining these values and achieving the plot; just read through the program’s assumptions and model used sections. You notice from the plot that it takes about 60 minutes to reach the peak levodopa concentration in plasma and that it is close to the baseline when you need to take another dose of levodopa. Furthermore, 2 of 3 peaks are very similar, and the third is lower due to using the controlled release form of levodopa. So this plasma time course, based on the amount of levodopa being used, is likely comparable to many PwP.
My plots of the daily take data are included below, with some comments– Levodopa plus the Rotigotine patch is my usual treatment plan. What is shown in the illustration on top is the data inserted into the program, the calculated data given by the following drawing underneath. Finally, some calculated values are given in the Table below this plot.
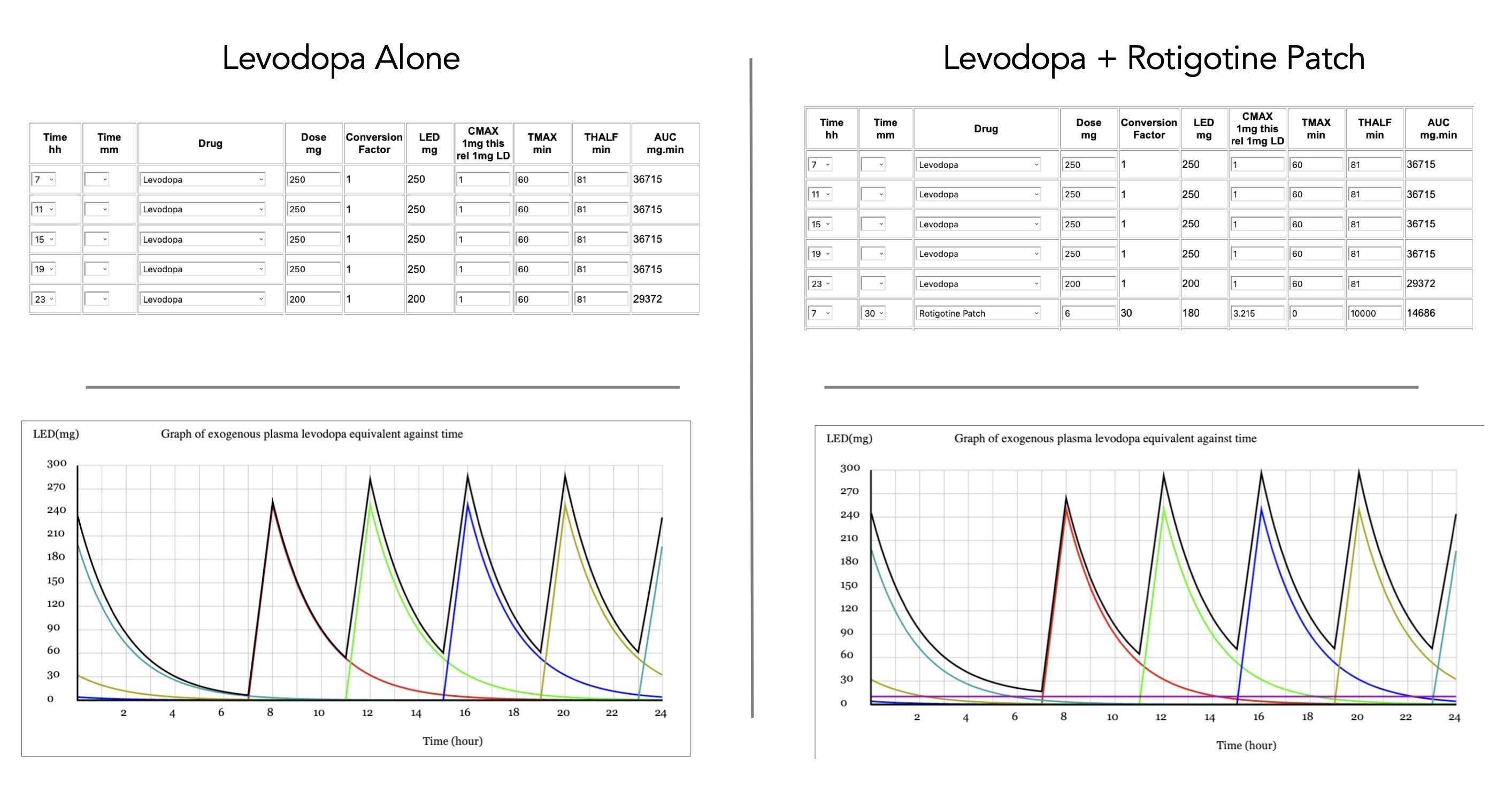
It is easier to compare/contrast the Table below entitled “Levodopa Equivalent Plasma Levels Under Varying Conditions” of four scenarios. The first two above compare my taking levodopa +/- the dopamine agonist patch (for my occasional forgetful self). At first, I thought leaving off the small amount of dopamine agonist in the patch did not account for much. However, the plasma Max, Mean, and Min are each about 10 mg LED lower with no patch than when including the Neupro patch. Clearly, all forms of levodopa make a difference.
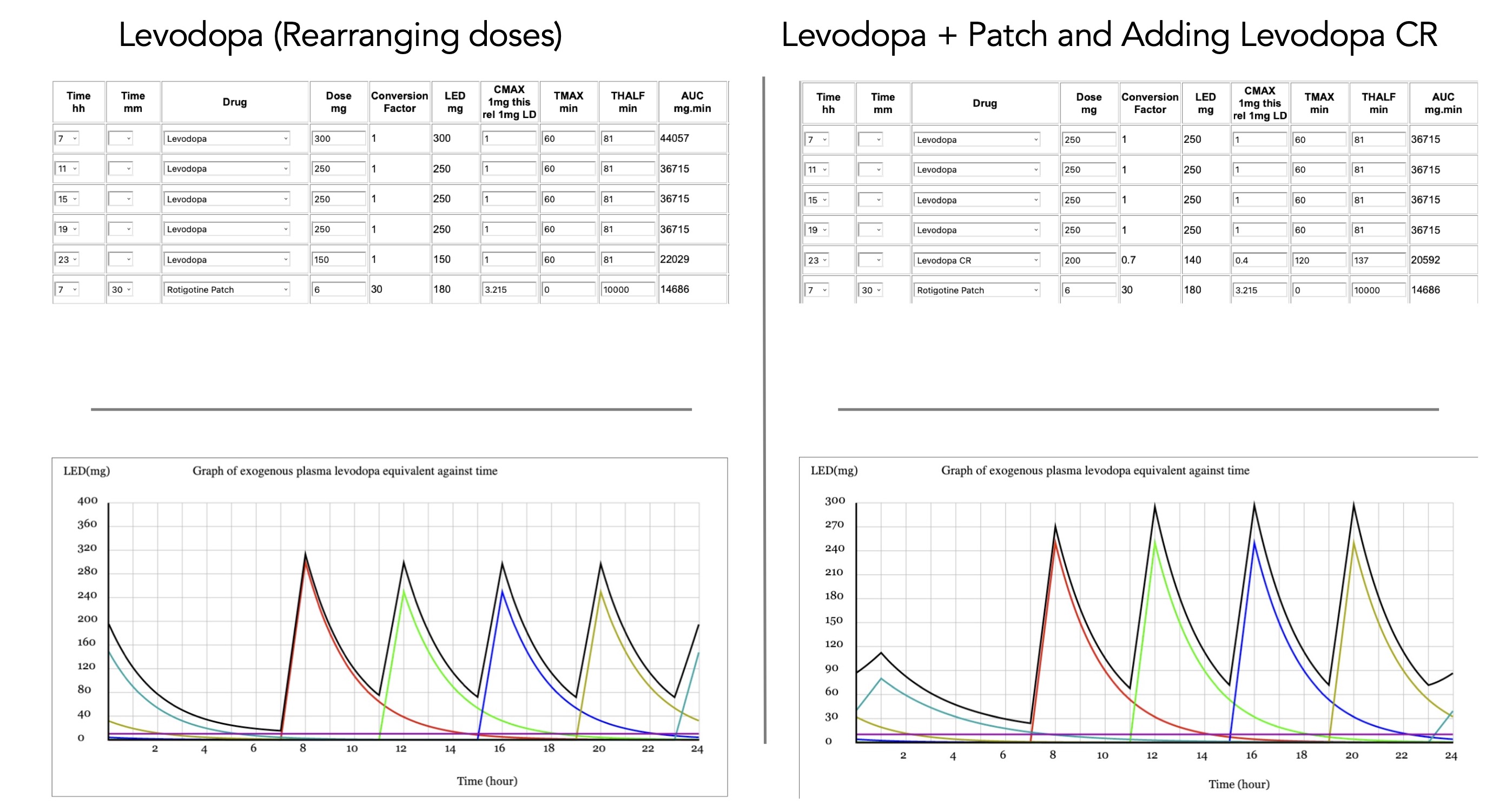
The additional two plots are both imaginary scenarios. First, at times, I have wondered if rearranging my doses might give me a better morning. Therefore, I redid the amount scenario slightly. Taking three tablets of levodopa (300 mg) at 7 AM reduced my final amount of levodopa at 11 PM to 150 mg levodopa (trying to maintain the same total amount of LEDD of 1380 mg. Interestingly, while the plasma Max increased from ~297 to ~313 mg LED while maintaining the same Mean value, the Min value was slightly less at 15.33 compared to 16.7 mg LED. Whether this would mean I might feel better in the early morning with that first dose of levodopa and about the same when I woke up the next day would only be realized if tested.
The other imaginary scenario would be to add levodopa CR as the final drug used in the evening. Its longer half-life would maintain a little more levodopa throughout the evening than levodopa IR. The data calculated for using the levodopa CR revealed such a pattern with a very similar plasma Max value, with an increased Min value, although the Mean value was slightly reduced. Again, only by trying this drug use scenario would one realize if there was any difference between the two scenarios.

“Success is almost totally dependent upon drive and persistence.” Denis Waitley
Dyskinesia Threshold: I have not tried the dyskinesia feature of the program since I have not started dealing with dyskinesia. However, it would seem relatively straightforward to input the data and see it plotted against one’s levodopa plasma values. Obtaining this information could benefit your physician’s altering your drugs when shown this data.
“Paralyze resistance with persistence.” Woody Hayes
Different Types of Drugs: Many other types of levodopa compounds are in use today therapeutically to treat Parkinson’s. And they are all listed here for you to plug into your own ‘imaginary’ plasma-based search. Maybe you have friends with Parkinson’s who are delighted by compound X, whereby you plug in some of these values and find potentially exciting results. But, again, this is the time to talk with your Neurologists about other possibilities for your therapy.
“Success is the sum of small efforts, repeated day-in and day-out.” Robert Collier
A Final Thought: Looking at these charts, one can easily see why staying on a strict schedule can go a long way to normalizing one’s day. Let’s say that missing a dose by 1-2 hr could interrupt one’s smooth sailing. Thus, being aware of the time each day is essential.
This is a set of ideal assumptions put into a program on a computer. It is not real life. It is not under stress or harsh conditions where residual endogenous dopamine might be consumed faster than usual. Again, looking at these plots, one can imagine how rapid dopamine consumption might challenge your levodopa-like product’s response during the day. And again, timing may say, you might consider taking the next dose a little earlier than usual. You know your body better than anyone else.
You might find this program helpful in calculating and knowing your daily plasma LED levels based on your medication regimen. In addition, learning new things about Parkinson’s, especially your own disorder, is always good.
*Medical Disclaimer– These blog posts contain advice and information related to health care. It is not intended to replace medical advice. It should be used to supplement rather than replace regular care from your neurologist. It is recommended that you seek your physician’s advice/approval before embarking on any new health plan or changes to your existing plan/routine.
“As long as you’ve done your best, making mistakes doesn’t matter. You and I are human; we will mess up. What counts is learning from your mistakes and getting back up when life has knocked you down.” Shawn Johnson
Cover Photo Image by Michael Zeuschner from Pixabay

Thanks for the calculation website. I have been doing this for myself, so I have a few questions. From the papers that I have, the levodopa curve for two 25/200 Sinemet is not 2xone 25/100 but seems to run into a rate limiting step; is this accurate? Also, in other papers, certain types of food delay the full delivery by ~ 3 hrs with a peak at ~4 hr; have you seen this? {I have} While we seem to have similar daily doses, mine is 1370 mg, I also take Entacapone 200 mg which seems to average dose over time; do you have info here?
LikeLike
Hi John, are you asking whether 1 pill with 200 mg levodopa has the same properties as 2 pills with 100 mg levodopa? In my mind, the rate limiting step is the absorption from the GI tract to the bloodstream leading to the brain. I would imagine that rate-limiting steps were part of the assumptions that guided the authors when creating their program. But simply thinking about it, 200 mg levodopa, whether in 1 pll or 2 should be roughly the same in their properties. Yes, certain foods would/could/may interfere with the absorption of levodopa and either delay or reduce the amount of levodopa available to your brain. But remember, this is not part of this program. It does not deal with complications of therapy, just the simple, take this amount, it gets to your bloodstream at approximately this amount. But you are absolutely correct, we must onsider our eating when taking levodopa-based products can make a difference. Now this is what I know about Entacapone. It is an inhibitor of COMT. It is combined with levodopa and carbidopa to treat the end-of-dose ‘wearing-off’ symptoms of Parkinson’s. So the category to use here would just be generic levodopa and enter the amount of levodpa in the Entacapone tablet you are taking. Again, the carbidopa and Entacapone have no entry here. Saying that “specific drugs” with documented half-lives are included here, maybe that value for Entacapone just needs to be added to the program? Thanks for the note John, Happy New Year! Frank
LikeLike
A year later and I’ve just come across your excellent website. I’m the person who wrote the graphing app.
On the specific question of whether two 100 mg levodopa (assumed with carbidopa) pills has the same effect as one 200 mg pill, at least as far as levodopa is concerned, the assumption used in the model is that doses are additive. So, in the pharmacokinetic sense for levodopa 2 x 100 = 1 x 200. But, if the two 100 mg regimen, was used in a different way with the 100 mg pills being taken at different times, the effect would be different.
Other drugs are treated differently. For instance, rasagiline is set to have a maximum effect at a daily dose of 1 mg (equivalent to 100 mg levodopa). Increasing the dose above 1 mg leaves the levodopa equivalent unchanged.
If anyone wishes to collaborate in this area, please get in touch. I think that it would be a reasonable goal to extend the app to include all major dopaminergics.
John
LikeLike