


“Come grow old with me. The best is yet to be.” William Wordsworth
“As long as I am breathing, in my eyes, I am just beginning.” Criss Jami
Introduction: Likely, everyone in the world has said the words “COVID-19 Pandemic” at some point since early 2020. From mid-February 2020 to December 2022, more than 324,000 publications on some aspects of COVID-19 were listed in PubMed Central, a remarkable number of papers in peer-reviewed journals. Therefore, I can proudly say that several of my publications from 2020-2022 either dealt specifically with COVID-19 infection and Parkinson’s or mentioned adapting to the COVID-19 pandemic in the classroom:
Hribar, Casey A., Peter H. Cobbold, and Frank C. Church. “Potential Role of Vitamin D in the Elderly to Resist COVID-19 and to Slow Progression of Parkinson’s Disease.” Brain Sciences 10.5 (2020): 284. Open access free download: https://www.mdpi.com/2076-3425/10/5/284
Hall, Mary-Frances E., and Frank C. Church. “Exercise for Older Adults Improves the Quality of Life in Parkinson’s Disease and Potentially Enhances the Immune Response to COVID-19.” Brain Sciences 10.9 (2020): 612. Open access free download: https://www.mdpi.com/2076-3425/10/9/612
McGreevy, Kristen M., and Frank C. Church. “Active Learning: Subtypes, Intra-Exam Comparison, and Student Survey in an Undergraduate Biology Course.” Education Sciences 10.7 (2020): 185. Open access free download: https://www.mdpi.com/2227-7102/10/7/185
Church, F.C., S.T. Cooper, Y.M. Fortenberry, L.N. Glasscock, and R. Hite. Useful Teaching Strategies in STEMM (Science, Technology, Engineering, Mathematics, and Medicine) Education During the COVID-19 Pandemic. Education Sciences. (2021): 11, 752. https://doi.org/10.3390/educsci11110752
Morowitz, J.M., K.B. Pogson, D.A. Roque, and F.C. Church. Role of SARS-CoV-2 in Modifying Neurodegenerative Processes in Parkinson’s Disease: A Narrative Review. Brain Sciences (2022): 12(5), 536; https://doi.org/10.3390/brainsci12050536
The information below is grouped around COVID-19, the immune system focused on older adults, and the interface linking or not linking Parkinson’s to COVID-19 infection.
“Age is an issue of mind over matter. If you don’t mind, it doesn’t matter.” Mark Twain
Living in the Presence of a Pandemic: The topic of this post relates to some health lessons and information* concerning those of us living with Parkinson’s amid aging adults and COVID-19. Our life is a series of lessons learned and how we adapted our lives, especially during challenging times.
Navigating the watery depths of COVID-19 required/requires effort for each of us to read, think, plan, and act upon how we manage(d) our day-to-day activities. There is no collective correct answer; only what you decide(d) to do is your proper response. Nevertheless, the world can recover from the COVID-19 pandemic if we support, share our understanding, and help each other learn and live.

“There is still no cure for the common birthday.” John Glenn
Introducing COVID-19 and SARS-CoV-2: In late 2019, a coronavirus was detected in Wuhan, China, as described in this report from the World Health Organization (WHO), https://www.who.int/china/news/detail/09-01-2020-who-statement-regarding-cluster-of-pneumonia-cases-in-wuhan-china. The WHO named the new virus severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) after similarities to SARS were found. The resulting disease caused by this virus was coronavirus disease 2019 (COVID-19). SARS-CoV-2, like SARS and Middle East Respiratory Syndrome (MERS), is a coronavirus that is thought to have originated in bats.
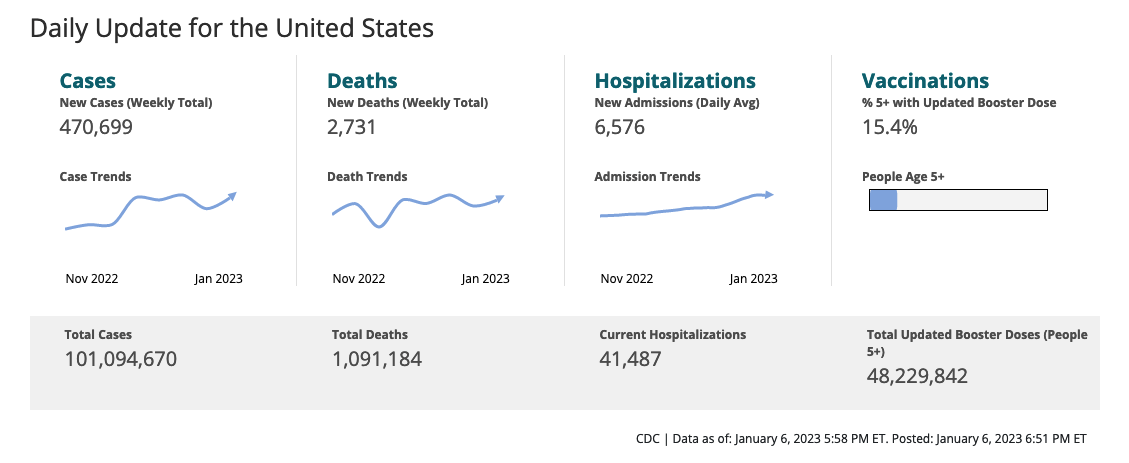
Over 1 million people in the USA have died due to SARS-CoV-2 infection (https://covid.cdc.gov/covid-data-tracker/#datatracker-home). Compare that to the death rates for Parkinson’s disease. From 1999 to 2017, age-adjusted death rates for Parkinson’s disease among adults aged ≥65 years increased from 41.7 to 65.3 per 100,000 population. (QuickStats: Age-Adjusted Death Rates for Parkinson’s Disease Among Adults Aged ≥65 Years — National Vital Statistics System, United States, 1999–2017. MMWR Morb Mortal Wkly Rep 2019;68:773. DOI: http://dx.doi.org/10.15585/mmwr.mm6835a6external icon. The two figures below are from these two sites, respectively.

“Old age is not a disease – it is strength and survivorship, triumph over all kinds of vicissitudes and disappointments, trials and illnesses.” Maggie Kuhn
10 Lessons Learned About the COVID-19 Pandemic, Older Adults, the Immune System, and Parkinson’s:
#1•The origin of the virus and mode of viral infection. A report by Worobey et al. (2022) suggested that a natural spillover emergence from a seafood wholesale market in Wuhan, China, was the most plausible starting point of the COVID-19 pandemic (Worobey M, Levy JI, Malpica Serrano L, Crits-Christoph A, Pekar JE, Goldstein SA, et al. The Huanan Seafood Wholesale Market in Wuhan was the early epicenter of the COVID-19 pandemic. Science. 2022;377 6609:951-9; doi: doi:10.1126/science.abp8715). Alternative and speculative theories exist and most implicate the institute nearby in that SARS-2 was either being tested there or, by negligence, it got released. There is no firm and credible evidence of the latter event happening, although there are a lot of alternative theories defending this notion.
According to the CDC, three pathways spread SARS-CoV-2: (i) Breathing in the air when close to an infected person who is exhaling tiny droplets and particles that contain the virus; (ii) Having these droplets and particles land on the eyes, nose, or mouth, and (iii) Touching the eyes, nose, and mouth with hands that have the virus on them.
#2•Initial response was quarantine (if symptoms were mild) and, for (many) weeks, shelter-at-home. The same SARS-CoV-2 was spread person-to-person from Wuhan, China, to Italy’s Lombardy region, New York City, and Seattle, Washington, USA. The world quickly became an incubator for viral spread. This quarantine/shelter-in-place plan gave us the fewest flu cases and deaths from flu in the past few years; the quarantine theory worked well for influenza (Rubin R. Influenza’s Unprecedented Low Profile During COVID-19 Pandemic Leaves Experts Wondering What This Flu Season Has in Store. JAMA. 2021;326 10:899-900; doi: 10.1001/jama.2021.14131.).
The so-called social distancing plan was 6 feet apart, good soap-hand-washing hygiene, and do not touch your face. Wearing a mask protected(s) you to some extent from others, especially where close contact is more prevalent. As the virus mutated in 2021-2022, heightened awareness spread, even in the USA.
Most governments have abandoned this protection strategy. Instead, most seem to be weighing the odds of new viral variants for infectivity and hoping for the best for all.
#3•Risks/odds of infection compared to other viruses. According to a recent report from Harvard University, about 50% of the USA claims to have been infected by SARS-CoV-2. Still, many of these infections have not been reported (https://www.hks.harvard.edu/faculty-research/policy-topics/health/half-us-population-has-had-covid-many-cases-are-going). Furthermore, many U.S. citizens say they have had COVID-19 more than twice.
For example, last January, with another spike of COVID-19 happening, we were given the option of either teaching live in a classroom or online by Zoom. Due to my age and Parkinson’s, I opted to teach the month of January online; this extended through February. Students were emailing me, reporting that they had gotten the virus (again) and that it was an excellent decision to teach online for a while. We moved to in-person after spring break, and only a few students reported COVID-19-positive. College-aged students could easily get infected with only a mild clinical scenario. Still, they were primed to spread the virus to others, potentially to their much older faculty members.
What is essential to recognize is that SARS-CoV-2 does not have the highest fatality rate compared to other emerging viral diseases like SARS and Ebola. However, SARS-CoV-2 has a high reproduction number, quickly spreads, and found an immunologically naive world population that has led to significant deaths compared to any other pandemic over the last 200 years.
#4•Risk of death based on age by decade and preexisting illnesses from COVID-19 infection. By December 2022, more than 1,000,000 deaths were reported in the USA due to SARS-CoV-2. Sadly and importantly, >93% of these deaths were in people aged 50 and older. Yes, chronic diseases, like cardiovascular disease, type 2 diabetes, and other chronic disorders, increase the risk of viral infection and, consequently, decrease the survival chances of the infected patient.

#5a•Is Parkinson’s a higher risk for severe COVID-19 infection? A person-with-Parkinson’s (PwP) might have some autonomic nervous system dysfunction. This significant jeopardy factor could potentially lead to severe COVID-19 disease. Significantly, PwP may have reduced lung function, and ARDS is part of the viral process, potentially making it difficult for the PwP if infected with SARS-CoV-2. However, definitive data regarding Parkinson’s and the risk of SARS-CoV-2 infection is not conclusive.
#5b•Does SARS-CoV-2 promote or accelerate Parkinson’s? This big unknown may have to wait 20-30 years to know the answer. Here’s a concern. SARS-CoV-2 has a neurotropic potential. That is, the virus can get to the brain. One of the first symptoms for many is the loss of smell. Sound familiar? In the review article, we wrote on the topic (Morowitz, J.M., K.B. Pogson, D.A. Roque, and F.C. Church. Role of SARS-CoV-2 in Modifying Neurodegenerative Processes in Parkinson’s Disease: A Narrative Review. Brain Sciences (2022): 12(5), 536; https://doi.org/10.3390/brainsci12050536), there is evidence that the virus can exacerbate existing symptoms of Parkinson’s. Possibly implicating inflammation pathways could assist the disease progression due to residual viral action. Furthermore, there is growing evidence that the immune system may contribute to this pathogenesis of Parkinson’s. SARS-CoV-2 may be an accelerant for someone’s existing Parkinson’s or help promote Parkinson’s or related parkinsonism disorder in a susceptible person.
#6•Vitamin D, older adults, COVID-19, and Parkinson’s. If you have Parkinson’s, a small amount of vitamin D3 daily is your friend. Many older adults have developed a deficiency of vitamin D3, and this vitamin has a pro-immune function by supporting the innate and adaptive immune systems. Furthermore, there is evidence that vitamin D3 has some function in slowing the progression of Parkinson’s. The paper we wrote about vitamin D3 (Hribar, Casey A., Peter H. Cobbold, and Frank C. Church. “Potential Role of Vitamin D in the Elderly to Resist COVID-19 and to Slow Progression of Parkinson’s Disease.” Brain Sciences 10.5 (2020): 284. Open access free download: https://www.mdpi.com/2076-3425/10/5/284), suggests that this vitamin could help maintain the immune system in older adults. Vitamin D3 helps those with Parkinson’s, which in the backdrop of the COVID-19 pandemic, could reduce the risk of viral infection.
#7•Immune System. We are learning that the immune system in older adults is not quite as functional as earlier in life. This suggests that the advent of sustained neuroinflammation would potentially predispose the person to develop Parkinson’s. The stimulus of the neuroinflammation would be the pathogenic alpha-synuclein bodies in neuronal cells. The immune imbalance is due to an overabundance of proinflammatory T-cells. These cells activate microglia (macrophage-like cells) to further propagate the proinflammatory microenvironment. Therefore, an individual infected by SARS-CoV-2 would tip the balance even further to a proinflammatory mix, possibly accelerating Parkinson’s in that person.
#8•“Long COVID.“ There is evidence that in a small percentage of people infected with SARS-oV-2, its symptoms persist long after the acute viral infection. This condition has been termed ” long COVID.” It can involve many other organs, not just the lungs. The symptoms of long covid include fatigue, dyspnea, cardiac abnormalities, cognitive impairment, sleep disturbances, symptoms of post-traumatic stress disorder, muscle pain, concentration problems, and headache. The concern from thinking about long COVID in the presence of Parkinson’s has been highlighted in a recent publication (Leta V, Rodríguez-Violante M, Abundes A, Rukavina K, Teo JT, Falup-Pecurariu C, Irincu L, Rota S, Bhidayasiri R, Storch A, Odin P, Antonini A, Ray Chaudhuri K. Parkinson’s Disease and Post-COVID-19 Syndrome: The Parkinson’s Long-COVID Spectrum. Mov Disord. 2021 Jun;36(6):1287-1289. doi: 10.1002/mds.28622. Epub 2021 Apr 28. PMID: 33890344; PMCID: PMC8250675.). The PwP described here had worsening motor-related symptoms, increased fatigue, “brain fog,” and increased carbidopa/levodopa therapy. They also contribute some of these features to the prolonged lockdown conditions and reduced access to medical care. The authors summarize that “post‐COVID clinical manifestations may result from a combination of new symptoms and lockdown as well as viral illness‐related worsening of preexisting PD features.”
#9•The effect of vaccination against COVID-19 and the herd effect. Herd immunity occurs when a large portion of a community (the herd) becomes immune to a disease. If enough people in the herd get immunized, the whole herd gains protection. The advent of large-scale vaccination against SARS-CoV-2 has successfully reduced the virus’s viral spread rate and the sheer number of deaths. The data from vaccination studies have shown that it may not completely block infection. Still, it has substantially reduced severe illness (that is, being hospitalized and dying). It builds a better immune response than those infected who think their natural immunity offers more protection; it does not. The CDC has a nice overview of the impact of the vaccine in providing a better outcome for COVID-19 infection (https://www.cdc.gov/coronavirus/2019-ncov/vaccines/vaccine-benefits.html).
#10•Do not believe everything you read. Like many things today, there is a lot of fake news on social media regarding the COVID-19 pandemic. Carefully choose what you read and believe from these posts. A good reference I found recently about such publications is from the School of Medicine at Yale University (https://www.yalemedicine.org/news/covid-19-infodemic).
“You’ll live to be a hundred if you give up all the things that make you want to.” Woody Allen
Conclusions: We have learned how better to live in the presence of the COVID-19 pandemic. Parkinson’s is an additional preexisting risk factor (although the epidemiological data is inconclusive). It also comes with our advancing age, yet another marker to be aware of concerning SARS-CoV-2 infection. The COVID-19 pandemic is not over.
A recent paper highlights the continued ill effects of reinfection of SARS-CoV-2. (Bowe B, Xie Y, Al-Aly Z. Acute and post-acute sequelae associated with SARS-CoV-2 reinfection. Nature Medicine. 2022;28 11:2398-405; doi: 10.1038/s41591-022-02051-3). We need a better strategy to offer total protection against all forms of SARS-CoV-2.
Until then, we continue to use common sense, good habits, and knowledge of COVID-19. Maintain a good history of vaccines and boosters when needed. Stay healthy, and be safe, my Parkinson’s friends.

“It is not all bad, this getting old, ripening. After the fruit has got its growth it should juice up and mellow. God forbid I should live long enough to ferment and rot and fall to the ground in a squash.” Josh Billings
*Please note this recurring medical disclimer: This blog post contains advice and information related to health care. It is not intended to replace medical advice. It should be used to supplement rather than replace regular care from your neurologist. It is recommended that you seek your physician’s advice/approval before embarking on any new health plan or changes to your existing plan/routine. The information in this blog post is as up-to-date as possible.
Cover photo Image by Roman Grac from Pixabay
