


“Behind every beautiful thing, there’s some kind of pain.” Bob Dylan
“You feel your strength in the experience of pain.” Jim Morrison
An Aging Population with Chronic Pain: The definition of chronic pain is pain that continues beyond the expected time of healing. Chronic pain can increase frailty, and it’s linked to falls, sleep disruption, depression, anxiety, and reduced physical function (to give just a few possible medical consequences of chronic pain). Rene Leriche described physical pain as, “Physical pain is not a simple affair of an impulse, traveling at a fixed rate along a nerve. It is the resultant of a conflict between a stimulus and the whole individual.”
You are not alone living with chronic pain. The number of older adults (65 years of age and older) is quickly growing, and those very old adults (85 years of age and older) with substantial pain and frailty are increasing even faster. Reports in the literature show that ~50% of community-based older adults describe pain daily. Moreover, this population of people does not also have Parkinson’s.
“Be patient and tough; someday this pain will be useful to you.” Ovid
Chronic Pain in Parkinson’s: You are not alone living with chronic pain in the presence of Parkinson’s. In the first medical description of Parkinson’s in 1817 (originally named Shaking Palsy or Paralysis Agitans), James Parkinson noted that pain was a symptom in the original groups of patients he observed (reprinted here: Parkinson J. An essay on the shaking palsy. J Neuropsychiatry Clin Neurosci. 2002;14: 223–236; to read this essay, click here).
Move to 2018, and it was found that people-with-Parkinson’s had significantly more pain than their age-match controls without Parkinson’s [see Rana et al. (click here to view paper) listed in the Literature Citation at the bottom]. Furthermore, Parkinson’s patients with symptoms of depression had significantly higher levels of pain compared to control patients without depression.
It is important to note that there are no long-term recommendations for managing chronic pain with Parkinson’s due to the absence of large-scale clinical evaluation/trials focused on chronic pain. However, there is some acceptance of a general plan that typically includes stretching/exercise, physical therapy, careful assessment of all drugs you are taking, and a careful re-evaluation of dopaminergic-based drug therapy. Let’s further describe this multidisciplinary approach to managing the symptom of chronic pain in Parkinson’s.
“Pain is the great teacher of mankind. Beneath its breath souls develop.” Marie von Ebner-Eschenbach
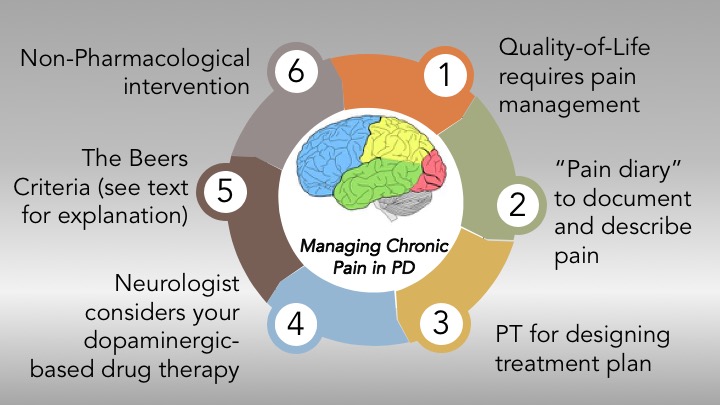
Managing Chronic Pain in Parkinson’s (see drawing above and the description below):
1) Quality of Life. Just because you may be an older adult with Parkinson’s does not mean you must live through chronic pain. Your quality of life will certainly be on a downward trajectory without some medical assistance/advice. Seek the help of your Neurologist or Internist/Family Practice Physician to devise a plan of action. Likely components of your management plan would include the following in #2-#6 below.
2) You may be asked to keep a “pain diary” to report the degree of pain, the amount of pain like when/where it occurs, and its frequency.
3) You may be referred to a Physical Therapist who would be able to provide stretches and exercises in an attempt to manage the pain if it is related to motor function. Again, your willingness to engage with your Physician is critical to establishing the need for such therapy.
4) Your neurologist would carefully consider the current treatment strategy (amount and time) of your dopaminergic-based drug therapy, especially if your pain evolves from a motor-related problem.
5) The Beers Criteria. The American Geriatric Society has developed a guide called the Beers Criteria, which is an essential tool to help your healthcare provider in improving medication safety in older adults. There are going to be a lot of pharmacological pain management choices for your Physician to consider. Importantly, in the aging body due to physiological changes and your current health conditions [Parkinson’s and any other coexisting health issue(s) and drug therapy] can be a formidable challenge to devising the best drug treatment plan. The Beers Criteria provides potentially inappropriate medications to be avoided in older adults. The Beers Criteria groups drugs in two categories: (a) drugs that should not be considered in older adults with specific disorders; and (b) drugs/classes of drugs that should be avoided in older adults due to unnecessary health risk or they are not effective and safer drugs are available. Here is the most recent free downloadable version of the Beers Criteria (click here); your Physician would likely use a more current version to develop your safe and effective treatment plan.
6) Non-Pharmacological intervention. Your Physician may recommend non-pharmacological remedies to manage your chronic pain including different forms of exercise (especially non-weight-bearing activities), music therapy, spiritual involvement, and relaxation therapy are just a few of many possibilities.
7) Remember, chronic pain is not a required part of normal aging. Albert Schweitzer once said, “The fellowship of those who bear the mark of pain: who are the members of this Fellowship? Those who have learnt by experience what physical pain and bodily anguish mean, belong together all the world over; they are united by a secret bond.” Keep engaged, try your best to manage your chronic pain in Parkinson’s. Seek the advice of your Physician to carefully develop your plan to try to remedy and reduce your chronic pain.
“Bad things do happen; how I respond to them defines my character and the quality of my life. I can choose to sit in perpetual sadness, immobilized by the gravity of my loss, or I can choose to rise from the pain and treasure the most precious gift I have – life itself.” Walter Anderson
Additional References:
Buhmann, C., N. Wrobel, W. Grashorn, O. Fruendt, K. Wesemann, S. Diedrich and U. Bingel (2017). “Pain in Parkinson disease: a cross-sectional survey of its prevalence, specifics, and therapy.” Journal of neurology 264(4): 758-769.
Ford, B. (2010). “Pain in Parkinson’s disease.” Mov Disord 25.
Ha, A. D. and J. Jankovic (2012). “Pain in Parkinson’s disease.” Movement Disorders 27(4): 485-491.
Lee, M. A., R. W. Walker, T. J. Hildreth and W. M. Prentice (2006). “A survey of pain in idiopathic Parkinson’s disease.” Journal of pain and symptom management 32(5): 462-469.
Rana, A. Q., A. R. M. Qureshi, A. Haris, M. A. Danish, M. S. Furqan, O. Shaikh, Z. Sarfraz and R. Rana (2018). “Negative impact of severity of pain on mood, social life and general activity in Parkinson’s disease.” Neurological research 40(12): 1054-1059.
Reid, M. C., C. Eccleston and K. Pillemer (2015). “Management of chronic pain in older adults.” bmj 350: h532.
Schnitzer, T. J. (2006). “Update on guidelines for the treatment of chronic musculoskeletal pain.” Clinical Rheumatology 25(1): 22-29.
Sophie, M. and B. Ford (2012). “Management of pain in Parkinson’s disease.” CNS Drugs 26(11): 937-948.
Tinazzi, M., C. Del Vesco, E. Fincati, S. Ottaviani, N. Smania, G. Moretto, A. Fiaschi, D. Martino and G. Defazio (2006). “Pain and motor complications in Parkinson’s disease.” Journal of Neurology, Neurosurgery & Psychiatry 77(7): 822-825.
Cover photo credit: https://pixabay.com/en/beach-winter-zingst-2072215/

Thanks, Frank, for sharing your knowledge with us. I have been experiencing chronic leg pain for at least 4 yrs. Was diagnosed and treated for Restless Legs, sciatica, also did PT. None of which helped. While discussing DBS for tremor with my neurosurgeon he said it sounded like dystonia and said DBS can address that. Have you heard anything like that?
LikeLike
Thanks for your note Karen. I’m sorry to hear about your leg pain; I would have hoped that Exercise combined with physical therapy would have helped you. And, I’m no expert on DBS. I would continue to have conversations with your neurosurgeon if he or she thinks it could help you (And any evidence available to support the recommendation). Best wishes, Frank
LikeLike