


“When I hear somebody sigh, ‘Life is hard,’ I am always tempted to ask, ‘Compared to what?'” Sydney J. Harris
“Comparison is the death of joy.” Mark Twain
Overview: Recently, I have presented two blog posts on COMT (Catechol-O-methyl transferase) Inhibitors: “COMT Inhibitors in Parkinson’s: Tell Me More, Tell Me More” (click here) and “Addendum to COMT Inhibitors in Parkinson’s” (click here). These two posts were primarily about entacapone.
For two months while taking entacapone, my highs and lows with carbidopa/levodopa were more level. I had lowered my daily take of carbidopa/levodopa by about 12%, and I was generally feeling more robust. Then, on week 10 or 11, I started having diarrhea that Imodium could control; nevertheless, it was constant until I stopped the entacapone. Come to find out, one of the adverse side effects of entacapone is diarrhea (I learned about this by going back and reading some of the original clinical studies). I took two months off, tried entacapone again, and the diarrhea returned in <48 hr. Thus, I stopped taking the COMT inhibitor, entacapone.
My new Neurologist has convinced me to try a different COMT inhibitor, opicapone (Ongentys, 50 mg capsule). Herein is a brief comparison of opicapone to entacapone.
“Make certain that your goals are not measured in comparison with others.” Denis Waitley
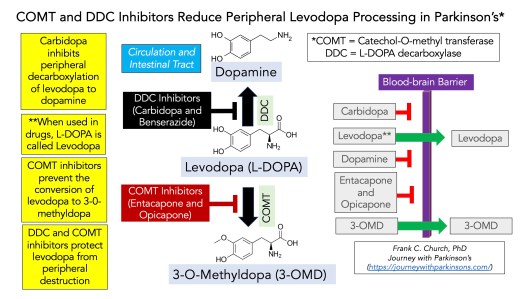
Role of Inhibitors to Allow Levodopa to Reach Blood Brain Barrier: LeWitt (2015) reported that unprotected levodopa is metabolized to dopamine throughout the body by an enzyme called L-DOPA decarboxylase (DDC). It is also referred to as peripheral L-amino acid decarboxylase. These DDCs would degrade ~70% of ingested levodopa. Thus, including a DDC inhibitor like carbidopa or benserazide blocks this process. It allows for a substantial amount of usable levodopa to reach the brain. Likewise, an enzyme named catechol-O-methyl transferase (COMT) provides a more minor yet measurable degradation of 10% levodopa to the 3-0-methyldopa (3-OMD) breakdown product. 3-OMD competes with levodopa binding at the blood-brain barrier, which would further reduce the amount of levodopa entering the brain. Ultimately, only about 1% of unprotected levodopa would reach the brain. The drawing below summarizes how COMT and DDC inhibitors protect levodopa and help it arrive in the brain to be converted to dopamine.
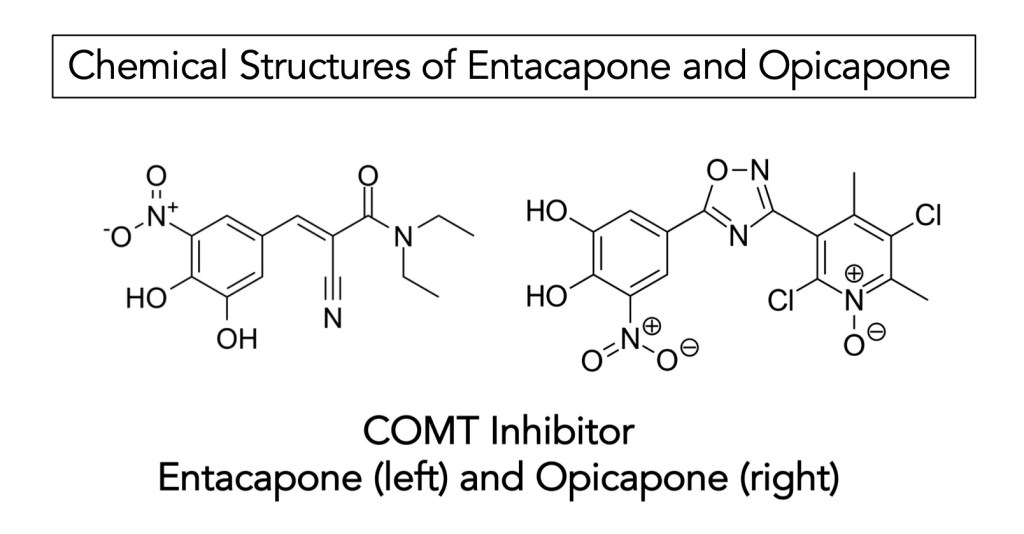
There are three COMT inhibitors currently available. The usual first choices are entacapone and opicapone. The typical dose of entacapone is 200 mg, usually three times per day (the maximum is eight times per day). The structure of opicapone is such that it is of higher affinity to COMT enzymes and has a longer half-life in circulation. Thus, opicapone is typically taken once daily (50 mg capsule), usually 1 hour after the last ingestion of carbidopa/levodopa and at least 1 hour before or after a meal/food. The third option would be tolcapone, but my Neurologist refrains from using it with her patients as it requires vigilant liver function testing. Generally, due to its generic status (and low cost), most people-with-Parkinson’s (PwP) would begin with entacapone. Although due to its superior pharmacokinetic properties and inhibitory properties, opicapone would be the better choice; however, opicapone is only available in the USA, Japan, and a few European countries.
Furthermore, opicapone is only available as Ongentys (not generic). Opicapone is substantially more expensive than entacapone (but will be worth it if it works). Finally, the chemical structures of entacapone and opicapone are given in the diagram below.
“Beware of little expenses. A small leak will sink a great ship.” Benjamin Franklin
Comparison of Opicapone to Entacapone: Several studies have directly compared the two COMT inhibitors, considering that motor fluctuations frequently contribute to healthcare resource utilization (HCRU) in PwP. With time, carbidopa/levodopa fluctuates during daily use after several years for treating Parkinson’s. Treatment with opicapone led to these differences when compared to entacapone:
•deceased HCRU;
•reduuced LEDD (levodopa equivalent daily dose);
•fewer outpatient neurology visits;
•no difference was seen in the use of sleep aids.
Adverse side effects of entacapone include diarrhea, nausea, vomiting, dizziness, lightheadedness, drowsiness, stomach upset, loss of appetite, trouble sleeping, headache, or dry mouth. Entacapone may also cause urine to turn a dark color.
Adverse side effects of opticapone include difficulty sleeping, sleepiness, abnormal dreams, dizziness, headache, low blood pressure, constipation, vomiting, dry mouth, muscle spasms, or hallucinations.
The most common side effect of entacapone and opticapone is dyskinesia due to dopaminergic excess.
COMT inhibitors were developed to overcome motor fluctuations by reducing the daily off-on time from extended use of carbidopa/levodopa.
COMT inhibitors improved UPDRS motor scores.
COMT inhibitors result in the reduction of the daily dose of carbidopa/levodopa.
Most clinical trials on COMT inhibitors measure quality of life (QoL). However, it is considered a secondary outcome, not a primary outcome. Thus, collecting such data and determining the power of an individual clinical trial is based on primary endpoint analysis, not secondary endpoints. Therefore, there is some variability of QoL in COMT inhibitor studies.
In an MDS evidence-based medicine review by Fox et al. (2018), all three COMT inhibitors were found to be effective in treating motor fluctuations in PwP due to off-on occurrence from carbidopa/levodopa.
“For like to like, the proverb saith.” Thomas Wyatt
Conclusions: This blog post was written to help me better understand how COMT inhibitors function and compare and contrast the adverse side effects of entacapone to opicapone. Since COMT inhibitors are used to control better the motor fluctuations from the use of carbidopa/levodopa over time, one would not use COMT inhibitor therapy without carbidopa/levodopa. And from reading the articles below, diarrhea is more of an issue for entacapone than it is for opicapone.
The treatment dilemma for most older adults with Parkinson’s who have this worsening off-on difficulty is as follows in the Table below. Most older adults may be at an upper limit of carbidopa/levodopa. Adding a dopamine agonist (DA) could improve motor function during the off-on period. DAs have a longer half-life and much higher LEDD. They are usually effective at controlling motor function, but they come with a whole set of emotional/psychological issues. Following DBS surgery, the PwP substantially reduces the daily amount of carbidopa/levodopa.

Increasing carbidopa/levodopa and adding a DA have both risk and merit. The most logical addition may be a COMT or monoamine oxidase B (MAO B) inhibitor, but not both simultaneously. MOA B inhibitors have not been discussed here; however, my Neurologist prefers the COMT inhibitor based on my lifestyle and energy level. The first choice would be entacapone due to its wide availability and low cost. Still, since I could not handle it, I have switched to opicapone. While more expensive and less widely available, the properties of opicapone are functionally superior to epicapone. I will keep you updated about my success (or not) in trying another COMT inhibitor, opicapone (Ongentys).
“Put light against light – you have nothing. Put dark against dark – you have nothing. It’s the contrast of light and dark that each give the other one meaning.” Bob Ross
Useful References:
LeWitt, Peter A. “Levodopa therapy for Parkinson’s disease: pharmacokinetics and pharmacodynamics.” Movement Disorders 30, no. 1 (2015): 64-72.
Greenwood, Jessica, Huy Pham, and Jose Rey. “Opicapone: a third generation COMT inhibitor.” Clinical Parkinsonism & Related Disorders 4 (2021): 100083.
Fabbri, Margherita, Joaquim J. Ferreira, and Olivier Rascol. “COMT Inhibitors in the Management of Parkinson’s Disease.” CNS drugs 36, no. 3 (2022): 261-282.
Ruottinen, H. M., and U. K. Rinne. “COMT inhibition in the treatment of Parkinson’s disease.” Journal of neurology 245 (1998): P25-P34.
Fox, Susan H., Regina Katzenschlager, Shen‐Yang Lim, Brandon Barton, Rob MA De Bie, Klaus Seppi, Miguel Coelho, Cristina Sampaio, and Movement Disorder Society Evidence‐Based Medicine Committee. “International Parkinson and movement disorder society evidence‐based medicine review: update on treatments for the motor symptoms of Parkinson’s disease.” Movement Disorders 33, no. 8 (2018): 1248-1266.
Harrison‐Jones, Glynn, Xiaocong Li Marston, Francesca Morgante, K. Ray Chaudhuri, Guillermo Castilla‐Fernández, and Valentina Di Foggia. “Opicapone versus entacapone: Head‐to‐head retrospective data‐based comparison of healthcare resource utilization in people with Parkinson’s disease new to catechol‐O‐methyltransferase (COMT) inhibitor treatment.” European Journal of Neurology 30, no. 10 (2023): 3132-3141.
Leta, Valentina, Daniel J. van Wamelen, Federico Aureli, Vinod Metta, Dhaval Trivedi, Pietro Cortelli, Carmen Rodriguez-Blazquez, Alexandra Rizos, and K. Ray Chaudhuri. “The real-life effect of catechol-O-methyltransferase inhibition on non-motor symptoms in levodopa-treated Parkinson’s disease: opicapone versus entacapone.” Journal of Neural Transmission (2023): 1-6.
Berger, Amnon A., Ariel Winnick, Jonathan Izygon, Binil M. Jacob, Jessica S. Kaye, Rachel J. Kaye, Elisa E. Neuchat et al. “Opicapone, a Novel Catechol-O-methyl Transferase Inhibitor, for Treatment of Parkinson’s Disease “Off” Episodes.” Health psychology research 10, no. 2 (2022).
Song, Zhaoming, Jie Zhang, Tao Xue, Yanbo Yang, Da Wu, Zhouqing Chen, Wanchun You, and Zhong Wang. “Different catechol-o-methyl transferase inhibitors in Parkinson’s disease: a bayesian network meta-analysis.” Frontiers in Neurology 12 (2021): 707723.
Regensburger, Martin, Chi Wang Ip, Zacharias Kohl, Christoph Schrader, Peter P. Urban, Jan Kassubek, and Wolfgang H. Jost. “Clinical benefit of MAO-B and COMT inhibition in Parkinson’s disease: practical considerations.” Journal of Neural Transmission (2023): 1-15.
Jost, Wolfgang H., and C. Brück. “Drug interactions in the treatment of Parkinson’s disease.” Journal of Neurology 249 (2002): iii24-iii29.
Kaakkola, Seppo. “Clinical pharmacology, therapeutic use and potential of COMT inhibitors in Parkinson’s disease.” Drugs 59 (2000): 1233-1250.
Fabbri, Margherita, Joaquim J. Ferreira, and Olivier Rascol. “COMT Inhibitors in the Management of Parkinson’s Disease.” CNS drugs 36, no. 3 (2022): 261-282.
Cover Photo Image by Engin Akyurt from Pixabay

Frank, I had been taking Ongentys(50mg) for over two years.about one month ago my Neurologist informed me that the medication will no longer be available. I now take Entacapone(200mg) with each 50-200 dose of Carbidopa-Levodopa, 4x per day. Here are my observations: my constapation has lessened (but no diarrhea); my dreams are less vivid; my on/off periods seam more defined; the on seams to last somewhat longer; however, my left hand tremor continues to the most difficult to control.
LikeLike
John, I thought I had replied to this note a day or ago, but evidently not. Thanks for your update about Ongentys being unavailable. I will check in with my Neurologist on Monday and seek her guidance. I searched the internet and found nothing, but your switching to Entacapone is definitely a real thing, as an alternative. I thought about contacting some GI folks that I know and posing the question “how could we get around the diarrhea caused by Entacapone?” The only thing I can think of is to grind up the tablets and stick the material under my tongue….but! Your description of your responses to a COMT inhibitor (constipation, dreams, etc.) are consistent with many others, which I guess is a good thing. Stay healthy! Frank
LikeLike
Thank you once again for sharing your knowledge, expertise and personal story, Frank. I’ve been learning a lot from your blog posts over the past months and years. I’m truly grateful to you.
LikeLike
Bill, thanks for your kind words. If I can make sense of it then I can try and relate it to everyone who reads the blog. But one never knows what the reader thinks about while reading a particular story, so I am very happy some of it makes sense to you. All-the best, Frank
LikeLike