


“Like cars, every relationship requires a bit of an occasional service, and fine-tuning should be compulsory.” Mariella Frostrup
“I actually credit Twitter with fine-tuning some joke-writing skills. I still feel like I’m working at it.” Steve Martin
Introduction: For those of you who have followed this blog for several years or more, I have typically gone to great lengths to describe the types and doses of therapy used. By definition, dopaminergic therapy (or dopamine replacement therapy) is the primary pharmacological treatment for Parkinson’s, which is designed to compensate for dopamine deficiency in the brain.
“People do not come into therapy to change their past but their future.” Milton H. Erickson
NOTE- If you want to read about the material on the topic of ‘fine-tuning’ of dopaminergic therapy, just skip down toward the bottom. Otherwise, enjoy reading the history lesson.
A History Lesson: It always seems when I discuss dopaminergic therapy, I realize that what “we” are taking drug-wise is as varied as “our” expression of symptoms. In other words, they can be very similar or somewhat different, and at times, they are very different from what I am about to discuss.
•The Start- A dopamine agonist (ropinerole). Moreover, what I will never forget is that after 2-3 years of not knowing what was wrong with me, about 30-60 minutes after swallowing that first dose, my body just totally melted, and my stiffness and clumsiness were gone, just gone.
•The Next 5 Years- As with most people with Parkinson’s, my need for ropinierole slowly increased; with time. I had worked up to taking 18 mg/day (3 x 2 mg tablets, 3 times per day). At this point, my Chapel Hill Neurologist (someone I greatly admired and respected) decided I needed to start taking Sinemet (Carbidopa/Levodopa). Therefore, I started both ropinirole and carbidopa/levodopa.
•The Ropinerole Taper- I reached a point where I was worried about the detrimental impact of a dopamine agonist; they are potent drugs with the capacity to influence your actions. I decided it was time to get off of Ropinerole, and my Neurologist agreed. Having written about Dopamine Agonist Withdrawal Syndrome (DAWS) (click here), I was worried that I could be in that minority of Parrkinson’s patients unable to get off of the dopamine agonist. Thankfully, I tapered off Ropinerole (click here).
•A Time for Sinemet- Carbidopa/levodopa (mostly known as Sinemet) is the best drug historically for treating the motor symptoms of Parkinson’s. A weakness of carbidopa/levodopa is its rapid metabolism; thus, it has a relatively short half-life when taken orally. At this point, the Chapel Hill Neurologist convinced me to add a dopamine agonist patch (NeuPro). The argument for using it was that it supposedly lacked the compulsive-behavior features of ropinerole and had a relatively long half-life in the body. Thus, NeuPro was added to my daily medication as a bridge to sustain my on time with regards to levodopa.
•Retirement and the Move to South Carolina- After ~40 years in Chapel Hill, I made the bold move to retire near Hilton Head Island in South Carolina. One of the biggest differences was getting health care, which had never crossed my mind before I moved. My SC-Neurologist is very talented, but she is overworked due to a lack of Movement Disorder Neurologists and a seemingly large number of retired folks here with Parkinson’s. Certainly, the proximity of Hilton Head Island’s beaches is wonderful, but a bleak picture regarding healthcare. It has taken me 3 years to get everything lined up for my medical care (it is all excellent now).
•Adding a COMT Inhibitor- Now approaching my 70’s, my new Neurologist wanted me to stop the NeuPro dopamine agonist patch and try a COMT inhibitor to prolong my levodopa. The idea was that if the COMT inhibitor prolonged levodopa’s half-life, I could reduce my daily Sinemet intake and also taper off NeuPro. Thus, I was excited by this possible change in dopaminergic therapy.
Started the COMT inhibitor entacapone, and I must say, it felt great over the first couple of weeks. It seemed to supercharge the levodopa, almost as if I were ‘spiking’ it with extra effect. Then, exactly two months into taking entacapone, I started with the most annoying and challenging diarrhea. Of course, it stopped when I stopped taking the entacapone. I started it again, and sure enough, the diarrhea returned. According to the manufacturer’s official handout, diarrhea after several months was a known side effect for some people.
My new Neurologist convinced me to try opicapone, another COMT inhibitor, and within a few weeks, Susan said that my personality had gotten really ‘weird’ on opicapone. So, using the baseball term, I was batting 0-for-2 on COMT inhibitors. You can read about my experience with COMT inhibitors (click here, then click here, and finally, click here).
•The ‘On-Off’ Battle with Carbidopa/Levodopa- There is nothing gentle about Parkinson’s; it is evil through and through. It is a disease that slowly progresses, and it never stops. The substantia nigra pars compacta is one of the two places where we have dopaminergic neurons, our cells that synthesize dopamine. It is expected that more than 50-60% of these neurons have died, leading to trouble with our motor symptoms. Many years ago, I depicted this phenomenon with grapes representing dopaminergic neurons (click here). Here they are again:
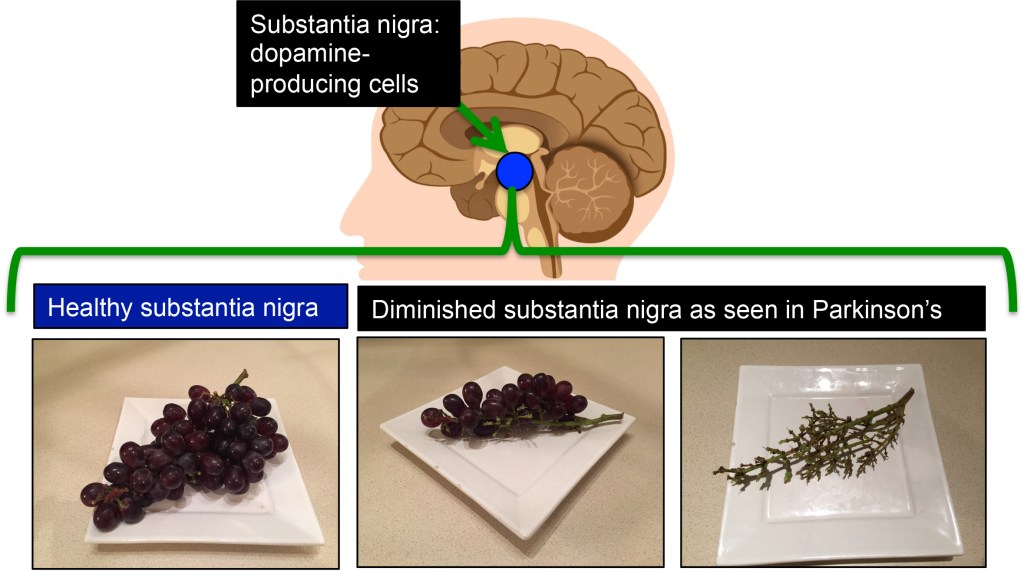
Imagine now: it has been 10 years or more, and you have fewer dopamine-producing neurons than before, and they are still diminishing. Interestingly, the striatum, which receives the dopamine made from these neurons. is maintained over the years to keep dopamine at a steady level. What does this mean? Over time, our carbidopa/levodopa dosing increases because fewer dopamine-producing neurons are slowly but steadily dying, and the supply of dopamine to the striatum may be rising with our doses, leading to things getting out of whack.
Chronic treatment with carbidopa/levodopa eventually leads to the development of motor complications, wearing-off issues, and dyskinesia in most patients with Parkinson’s. The extremes of the ‘On-Off’ can produce a levodop-induced dyskinesia during the ‘on’phase and then a crippling Parkinsonism [including the really cruel freezing of gait (FOG)] during the ‘off’ phase. Yes, I was starting to feel the consequences of the on-off phase of my carbidopa/levodopa, as FOG would occur if I allowed the Sinemet to bottom out (see my post about FOG).
•The Crexont Experience- I may be the worst kind of patient, party, because I refuse to accept my symptoms as the endpoint to my approach to therapy. I am sure it is annoying to my SC-Neurologist, but she listens to my comments and responds to my emails. I am not challenging her expertise and experience, but I am just convinced that one person with Parkinson’s may need a very personalized treatment strategy,
I started reading Parkinson’s papers on how to increase the half-life of levodopa. That was the idea my SC-Nurogist tried with the COMT inhibitors; they worked well, but my genetic makeup did not tolerate them.
This led me to study the extended-release forms of levodopa. I first tried the controlled-release version of Sinemet (and since it was generic, my insurance made it almost free), and oh my, it totally messed up my on-off cycle; it seemed I was just not getting any dopamine in my body. This was most confounding, but my SC Neurologist said it was ‘different’ than traditional ‘immediate-release’ Sinimet (that is, the standard carbidopa/levodopa, 25 mg/100 mg ratio). I quickly stopped taking the controlled-release Sinemet.
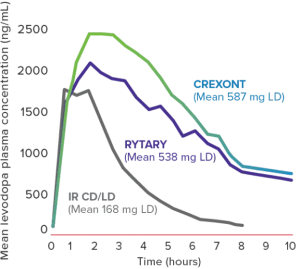
The path changed, and I started reading about extended-release forms of carbidopa-levodopa, named Rytary and Crexont (originally named IPX203, if you are interested in its history in medical journals). When compared to immediate-release carbidopa/levodopa vs. extended-release carbidopa-levodopa Rytary or Crexont (IPX203), Rytary gave an extra ~1.5 hours of on-time, and Crexont provided an extra ~2 hours of on-time (see this blog for further details). You frequently see figures like this when comparing these levodopa-containing drugs. Clearly, Rytary and Crexont did an excellent job of prolonging the half-life of levodopa.
I suggested to my SC-Neurologist that I would like to try Crexont. By now, she did not doubt my rationale or reasons. First, we had to convince the insurance company that a new drug, an upper-tier pay rate drug, would be good for my Parkinson’s. They agreed, and my 90-day dose was now $64 compared to ~$10 for a 90-day supply of Sinemet. I started taking it about a month before my first hip replacement surgery last May, 2025, and it worked well. Crexont did exactly what the company said it could do: give one significantly more on time than traditional carbidopa-levodopa.
•Tapering off and getting back on the NeuPro Dopamine Agonist Patch- There is something magical about turning 70 years of age and being told one should stop taking their dopamine agonist. The literature is filled with papers that say it is not safe for patients over 70 to be taking a dopamine agonist. Digging deeper, there is some evidence of drug interactions that occur with dopamine agonists that seem to be magnified by advanced age. And further instances of adverse personality changes from the dopamine agonist. However, here is my argument: dopamine agonists really work to reduce motor symptoms, and my other drugs (statins, etc.) have been interacting with a dopamine agonist for over a decade with no ‘badness’ occurring. So I agreed last fall to taper off the NeuPro path from 6 mg patch/day, 4 mg patch/day, 3 mg patch/day (I made these by cutting some 6 mg patches in half), and finally to 2 mg patch/day. I went slow and did each stage for a month.
The Crexont was doing its job, and most of the motor symptoms were under control. A month after stopping the NeuPro patch, I noticed my voice seemed weaker, at times when I talked, at times I sounded ‘drunk’, and my jaw’s slight tremor was acting up at times. I read more about age and dopamine agonists and decided that the benefit to my quality of life of going back on a 2 mg patch/day of NeuPro outweighed the potential bad problems. And my SC Neurologist totally agreed. So far, so good, the small dose of dopamine agonist in the NeuPro patch reverses the problems I was having without the dopamine agonist.
•Fine-tuning Crexont- Okay, it is the first day of February, 2026, I am two weeks out of my second hip replacement surgery (and yes, it is going well, I am on track to play golf again in March, 2026). How Crexont extends the on-time of levodopa is not fully understood. This uncertainty reminds me of my favorite line from the movie ‘Shakespeare in Love,’ where Philip Henslowe says,“I don’t know. It’s a mystery.” In November-December of last year, I started thinking about Crexont and wondered whether I could improve the dosing schedule I was on. I had several issues.
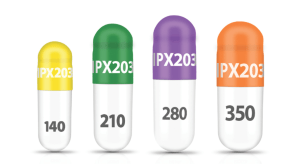
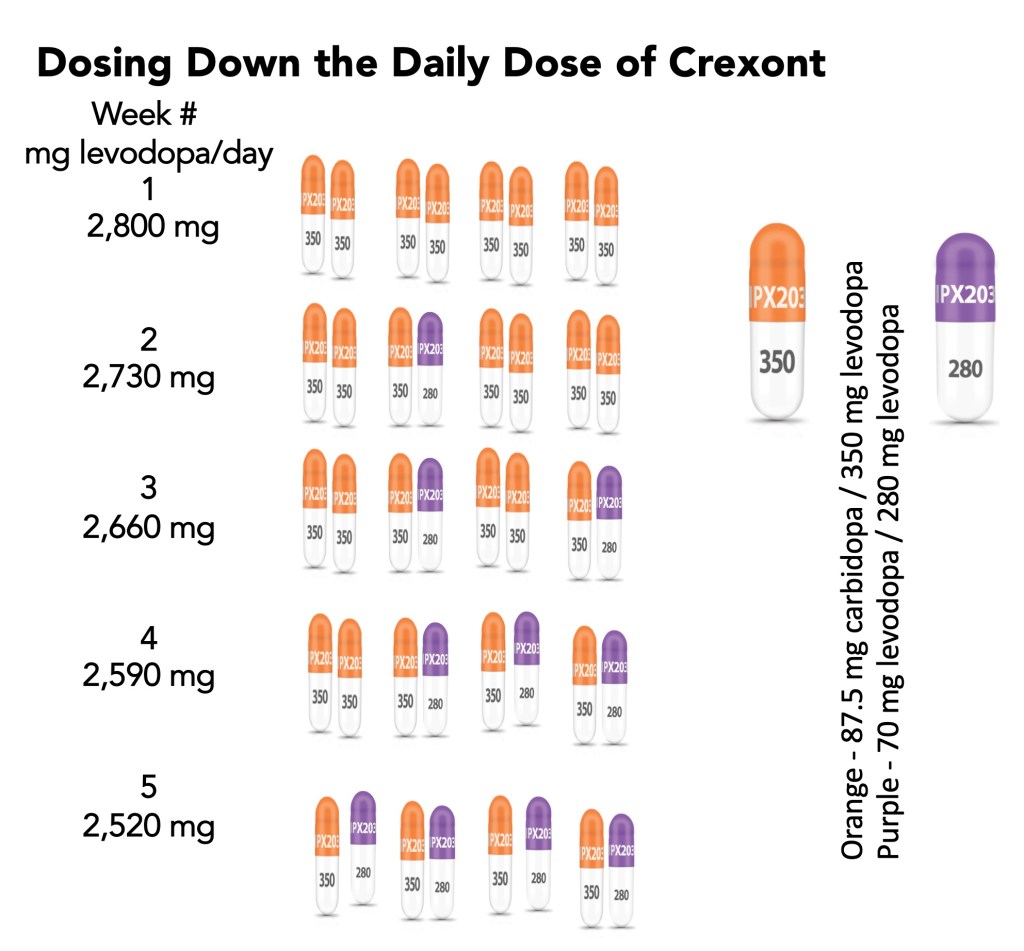
#1-My dose of Crexont causes levodopa-induced dyskinesia- Crexont comes in four doses of levodopa (see above). The conversion generally accepted for calculating how much Crexont I should take compared to how much carbidopa/levodopa I was taking seemed enormous. I was taking 2.5 tablets of carbidopa/levodopa (25 mg/100 mg) 5 times per day, which was 1300 mg of levodopa/day. Conversion to Crexont meant taking 2 capsules of Crexont (carbidopa/levodopa, 87.5 mg/350 mg) 4 times daily. The total Crexont dose was 2800 mg of levodopa per day, or 2.2 times my traditional dosage.
#2- Crexont has decreased the frequency of FOG, but when you go off Crexont, it would appear to be no better than traditional carbidopa/levodopa. Everything told about Crexont is absolutely true. There is a special kind of casing on the capsule: ~1/3 of the carbidopa-levodopa is released immediately, and the remaining 2/3 of the drug is somehow treated to have a longer half-life in blood plasma, acting better than the traditional carbidopa/levodopa.
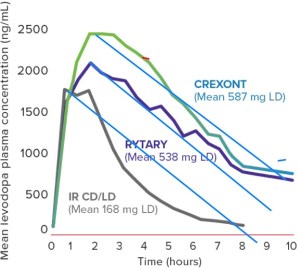
#3- Thus, without its special coating and protective shell, Crexont is still just carbidopa/levodopa, and the decay-time should be similar to traditional carbidopa/levodopa. Look at a similar figure where I have tried to highlight the off-rate of traditional Sinemet, Rytary, and Crexont. What it tells me is that once the carbidopa-levodopa is released from all its ‘protective’ coverings/coatings, the decay rates are all similar to one another. My experience with Crexont tells me I can go 4-6 hours between doses, depending on what I am doing (for example, sitting at my desk typing or out hitting golf balls). The one true advantage Crexont has is taking the last dose in the evening, then sleeping for 5-9 hours; you wake up and can typically feel okay.
#4- Optimizing Crexont- I was convinced that I was taking too much Crexont, especially since I had never had any dykineisa before. When it happens, it is a most unusual feeling. So I asked my SC Neurologist if I could do an experiment and try to replace some of my 350 mg capsules of Crexont with 280 mg capsules of Crexont? She smiled and said, ” Sure, let’s do it.” I decide to give each new dose a week for my body to get used to it. The scheme that I followed is illustrated below. The battle is to take enough Crexont that it controls my motor symptoms effectively without causing levodopa-induced dyskinesia. Then, while it is coming down, does it cause me to express my Parkinsonism, for me, that would be FOG.
Currently, I am still fiddling with it, primarily because I know what each feels like, the sudden surge of Crexont reaches some point in my circulation (or brain), and the dyskinesia starts, but then it stops, and at some point, I can sense the off-phase crosses a point that my gait freezes up. It is truly a balancing act that your body is the fulcrum, and the pivot points swing through extremes ranging from dyskinesia to Parkinsonism.
“Medication should never be considered the only tool for helping a person.” Temple Grandin
An Important Paper: I still read a lot of science articles. I ran across the following paper from 2013, yes, it is not current: Warren Olanow, C., et al. “Factors predictive of the development of levodopa‐induced dyskinesia and wearing‐off in Parkinson’s disease.” Movement Disorders 28.8 (2013): 1064-1071. It is quite a remarkable paper. This is a detailed study, with many conclusions and relevant comments about dosing of dopaminergic drugs:
•”Levodopa (L-dopa) is the gold standard for treatment of Parkinson’s disease (PD), and no medical or surgical therapy has been shown to provide superior anti-parkinsonism benefit. However, chronic L-dopa treatment is associated with the development of motor complications (wearing-off episodes and dyskinesia) in the majority of patients.”
•”The development of an L-dopa treatment approach that provides the benefits of the drug with a reduced risk of motor complications remains a major unmet need.”
•”The risk of developing dyskinesia or wearing off was closely linked to L-dopa dose.”
•”The current results suggest that physicians should use the lowest dose of L-dopa that provides satisfactory clinical control to minimize the risk of both dyskinesia and wearing-off.”
“Medication without explanation is obscene.” Toni Cade Bambara
Closing Thoughts: If you are struggling with the dose of your dopaminergic therapy, and if your Neurologist is willing to let you experiment with your dosing of drugs, then carefully move forward and see if you can optimize the dose. Ask your Neurologist for help; they are on your side, and they should assist in figuring out the most appropriate therapy (and amount) for you.
In many ways, Crexont is attempting to be that better drug, but I think it will take a very specific and directed trial to get the correct dose. I really like the concept of using the four different amounts of levodopa packaged in Crexont, seeking the best dose could truly balance the extreme differences between dyskenesia (too much levodopa) and wearing-off (too little levodopa).
Finally, I apologize for such a long post. I fely the need to write something, and I just kept going and going and going.
“About all you can do in life is be who you are. Some people will love you for you. Most will love you for what you can do for them, and some won’t like you at all.” Rita Maye Brown
